Lecture Code : PL02-S1
Session Name : Plenary Lecture 2
Session Topic : Plenary Lecture 2
Date & Time, Place : June 12 (Fri) / 12:50-13:40 / Auditorium, 3F
Cardio-Kidney-Metabolic Syndrome
Peter Rossing
Steno Diabetes Center Copenhagen, University of Copenhagen, Denmark
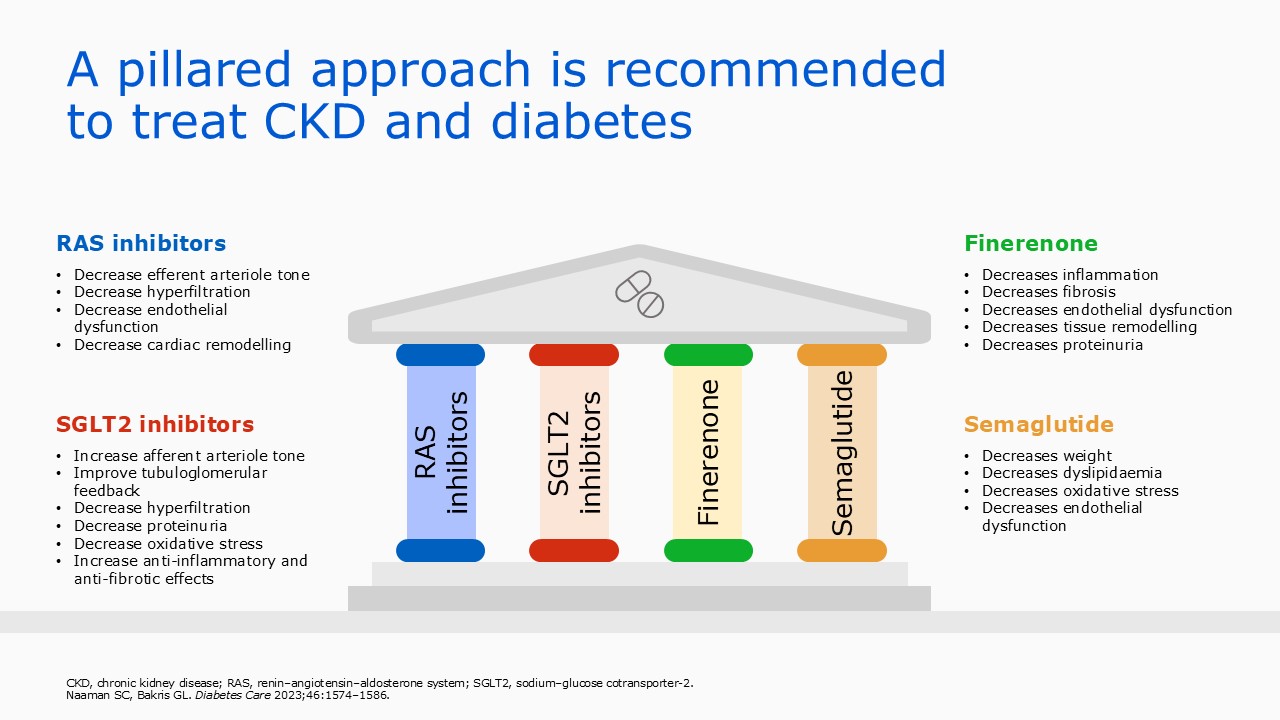
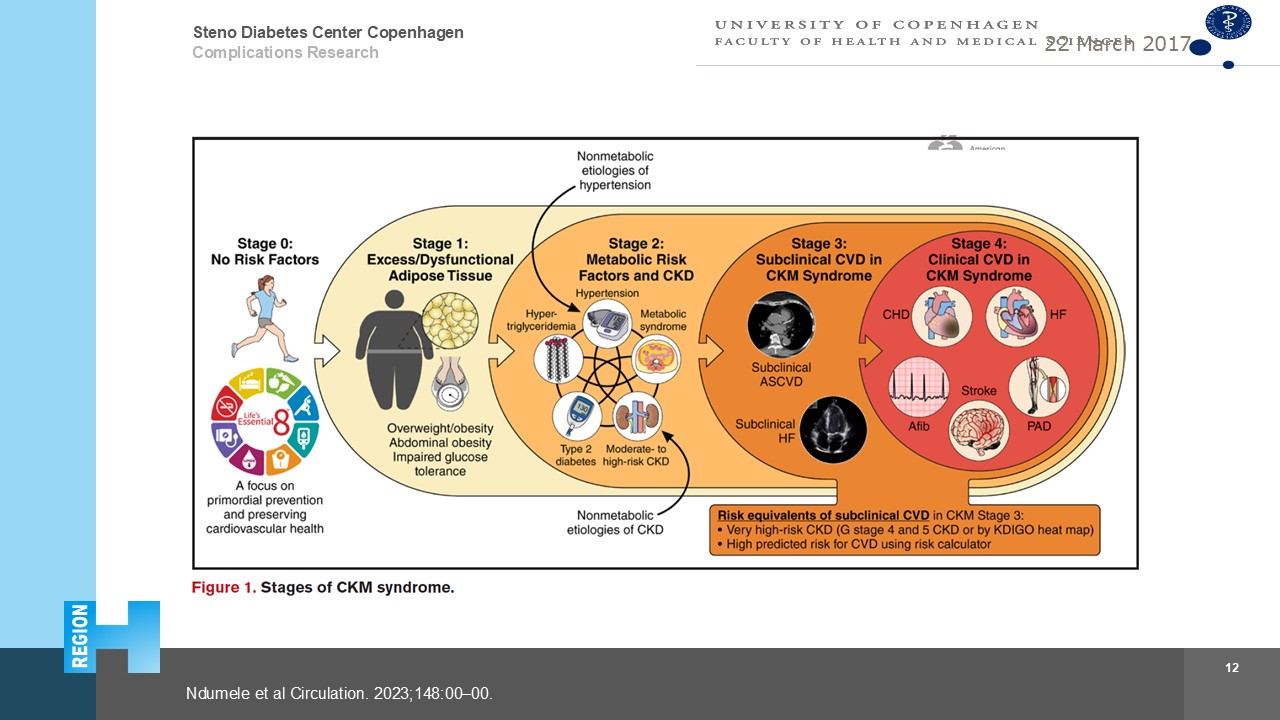
We have an epidemic of people living with overweight, approaching 1 billion people globally, and as a consequence we have a rise in diabetes incidence, and hypertension and this leads directly and indirectly to an increase in people with chronic kidney disease now almost 840 million people and cardiovascular complications and early mortality. The overlap between cardiovascular disease including heart failure and obesity diabetes, and CKD is striking. On the other hand we have never been in a better place to combat these complications. It starts with lifestyle interventions, but then blocking the renin angiotensin system, treating with SGLT2 inhibitors and Glucagon like peptide 1 receptor agonists and modulators of aldosterone (mineralocorticoid receptor antagnonists and aldosterone synthase inhibitors) have been demonstrated to benefit patients with cardio-kidney-metabolic syndrome, delay progression and reduce mortality. This has been termed pillars of therapy. The question is then how to apply? should everybody have all 4 pillars, or should clinical characteristics, or biomarkers guide thearpy, or should be aim to normalize urinary albumin excretion as a guide for intervention? THis is not clear at the moment, but we are gaining more and more evidence, and as an example the CONFIDENCE study demonstrated that nonsteroidal MRA finerenone, as well as SGLT2i empagliflozin reduced albuminuria 30 %, but the combination reduced albuminuria 53% suggesting combination is associated with better protection.
It all starts with screening and diagnosis, and current screening rates for CKM should be optimized to allow early intervention
Keywords: diabetes, cardio kidney metabolic, glp-1 ra, sglt2l
rossing 2026 hypertension ckd.jpg
rossing 2026 hypertension ckd.jpg