Lecture Code : PG02-S1
Session Name : PG Education 2 - Fluid & Electrolyte
Session Topic : PG Education 2 - Fluid & Electrolyte
Date & Time, Place : June 11 (Thu) / 10:30-12:00 / Room 2 (GBR 102), 1F
Salt Wasting vs SIADH: Hyponatremia with Volume Clues
Seon Ha Baek
Dongtan Sacred Heart Hospital, Republic of Korea
1. Strategic Importance: The Hyponatremia Dilemma
Hyponatremia is the most pervasive electrolyte disorder in clinical medicine, affecting 15% to 30% of hospitalized patients. Despite decades of study, the differential diagnosis between the Syndrome of Inappropriate Antidiuresis (SIAD) and Salt Wasting remains a "classic yet controversial" pivot point in nephrology.
The challenge lies in the fact that both SIAD and Salt Wasting present with a nearly identical biochemical signature: hypoosmolar hyponatremia, concentrated urine, and elevated natriuresis. However, they represent diametrically opposite volume states.
Although distinguishing SIAD from salt wasting is difficult, it is clinically crucial; moreover, the two etiologies may occur sequentially in the same patient as causes of hypoosmolar hyponatremia. There is no fixed diagnosis, and daily reassessment of fluid balance and urine output is essential.
2. Divergent Pathophysiology: Water Retention vs. Primary Sodium Loss
At the core of the dilemma is a fundamental physiological divergence: SIAD is a state of primary water retention, while Salt Wasting is a state of primary natriuresis. (Table 1)
3. The Diagnostic Challenge: Deciphering Volume Clues
Physical examination remains notoriously unreliable, with accuracy for volume assessment at only 47-48%. We must rely on objective biochemical markers while remaining cognizant of their limitations.
BUN/Cr Ratio: While a ratio >20 suggests hypovolemia, we must be wary of "distortion factors." Steroid use, high-protein diets, and gastrointestinal bleeding can falsely elevate this ratio, masking the true state.
CVP Thresholds: In critical care, a CVP <6 cm H2O strongly indicates C/RSW, whereas 6–10 cm H2O is typical of SIADH.
POCUS: The "second stethoscope" is essential for measuring IVC diameter and the collapse index to confirm plasma contraction.
Emerging Markers: Beyond urate, the Fractional Excretion of Phosphate (FEPhos) is showing promise as a secondary marker for proximal tubular dysfunction in C/RSW.
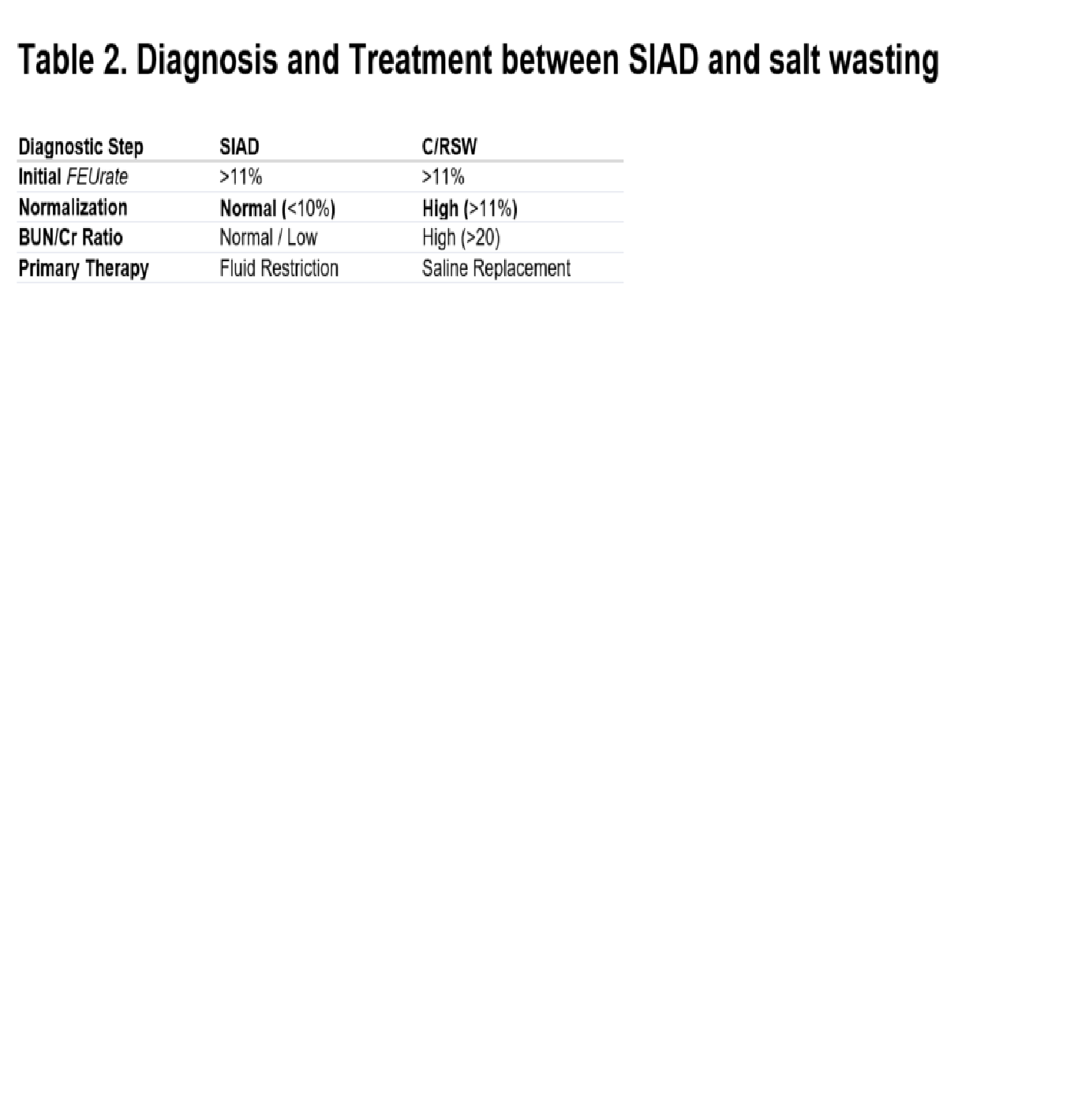
4. Fractional Excretion of Urate (FEUrate): The "Normalization Test"
Urate handling is the most sensitive proxy for proximal tubular function. Because the proximal tubule is the primary site of HPRWSP activity and volume-driven sodium handling, FEUrate serves as our most reliable diagnostic tool.
The Normalization Test Protocol
Initial State: During the hyponatremic phase, both SIADH and C/RSW present with an elevated FEUrate>11%.
Post-Correction (Isotonic Saline):
In SIAD: Once the relative volume expansion is corrected, FEUrate normalizes to <10%.
In C/RSW: Because the defect is a primary tubular impairment (driven by HPRWSP), FEUrate remains elevated (>11%)
5. Conclusion:
The Clinician’s Diagnostic Algorithm
Step 0: Exclude Pseudohyponatremia. Check for hyperglycemia and hyperlipidemia before proceeding.
Step 1: Confirm Hypoosmolarity. sNa<135, sOsm<275 mOsm/kg.
Step 2: Assess Proximal Function. Measure initial FEUrate.
Step 3: Analyze Volume Status. Evaluate CVP, POCUS, and BUN/Cr (accounting for steroids/GI bleeding).
Step 4: The Pivot. Perform the Normalization Test. If FEUrate remains >11% post-correction, it is C/RSW.
Keywords: Hyponatremia, SIAD, Salt wasting, FEUrate, Volume assessment
Table 1.png
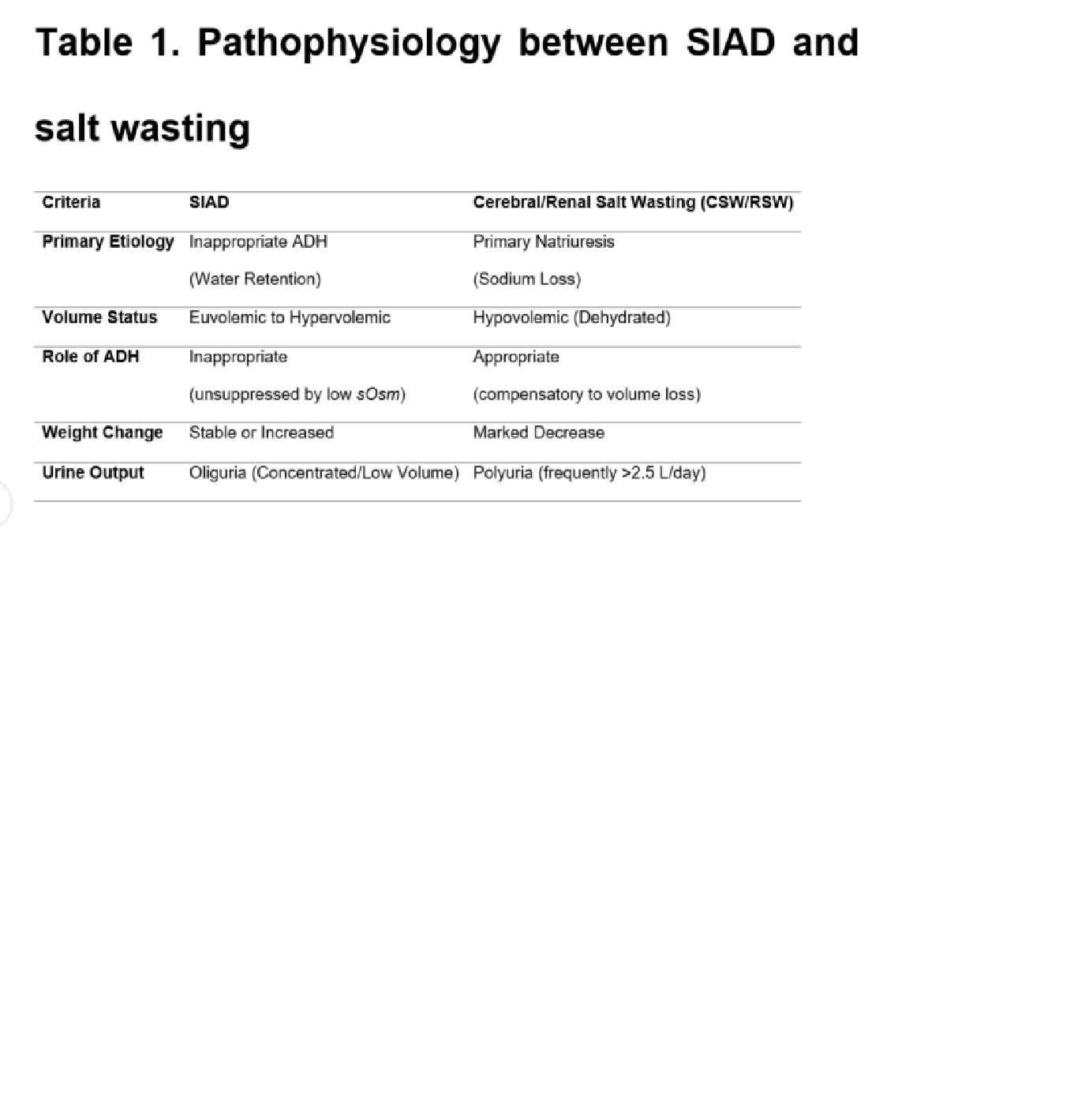
Table 1.png