Lecture Code : PA01-S1
Session Name : Pathology
Session Topic : Pathology
Date & Time, Place : June 11 (Thu) / 13:00-14:30 / Room 1 (GBR 101), 1F
Overview of MPGN: Transition from Morphological to Etiological Classification
Ryuji Ohashi
Nippon Medical School, Japan
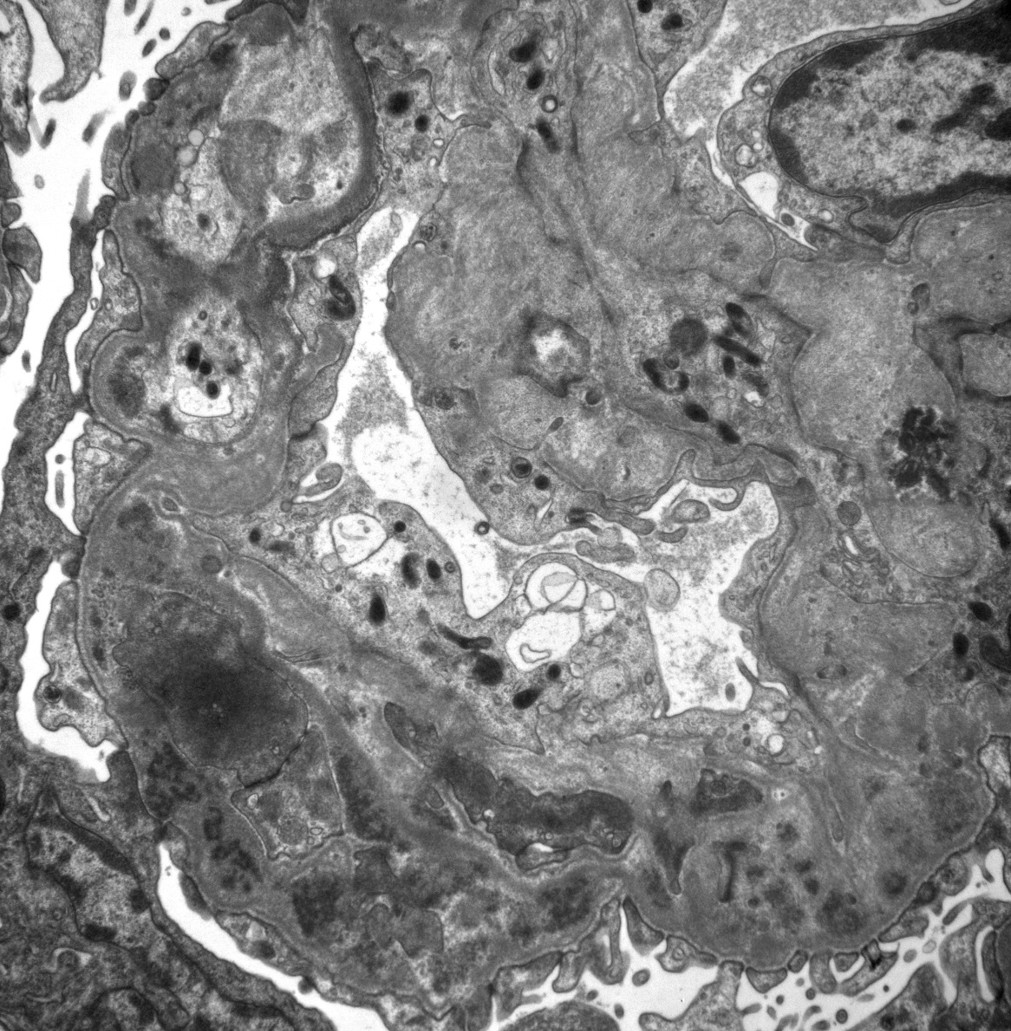
Membranoproliferative glomerulonephritis (MPGN) was initially recognized as a glomerulonephritis exhibiting proliferative changes in mesangium and glomerular capillary walls often accompanied by mesangial interposition under a light microscope. With the development of immunofluorescence (IF) and electron microscopy (EM) in the 1960s and 1970s, MPGN was further classified into types I, II, and III based on the pattern of alterations of glomerular basement membranes (GBM). MPGN type I is characterized by double contour of GBM and mesangial interposition (Fig1). Electron dense deposit (EDD) of peripheral capillary walls is mainly localized within subendothelial regions (Fig2). MPGN type II, now termed as dense deposit disease (DDD), is characterized by ribbon-like hyperdense deposits occupying lamina dense of GBM. MPGN type III can be subdivided into Burkholder and Strife & Anders types based on EM findings. Burkholder type is characterized by subepithelial EDD and fairly preserved GBM architecture. Strife & Anders type shows disruption of GBM associated with subendothelial and intramembranous EDD. At that time, MPGN was a pathological diagnostic term, but it was also recognized as a clinical entity. As etiological analysis progressed, some diseases diagnosed as MPGN were found to be caused by abnormalities in complement regulation, leading to the proposal of C3 glomerulopathy. Currently, classification is based on the deposition patterns of immunoglobulins and complements observed by IF. In other words, etiological backgrounds are more emphasized in order to design the treatment plan. Once morphology of MPGN is determined, it can be broadly classified into three categories: 1. those with predominant immunoglobulin deposition, 2. those with predominant complement deposition, and 3. those with no dominant deposition of either. Category 1 includes kidney diseases associated with autoimmune diseases such as lupus nephritis, diseases associated with infections such as HBV, HCV and parvovirus, and monoclonal immunoglobulin deposition disease. Proliferative glomerulonephritis with monoclonal IgG deposition is a disease mimicking immune-complex glomerulonephritis. Cryoglobulin glomerulonephritis, as an HCV-related disease, is also included in this category. Category 2 is represented by C3 glomerulopathy, which is further reclassified into C3 glomerulonephritis and dense deposit disease based on EM findings. Category 3 includes thrombotic microangiopathy, diabetic nephropathy and etc. In this lecture, I would like to provide an overview of the history and evolution of MPGN diagnosis from the perspective of a pathologist.
Keywords: MPGN, C3 nephropathy, dense deposit disease, complement regulation, monoclonal immunoglobulin
Fig1.jpg
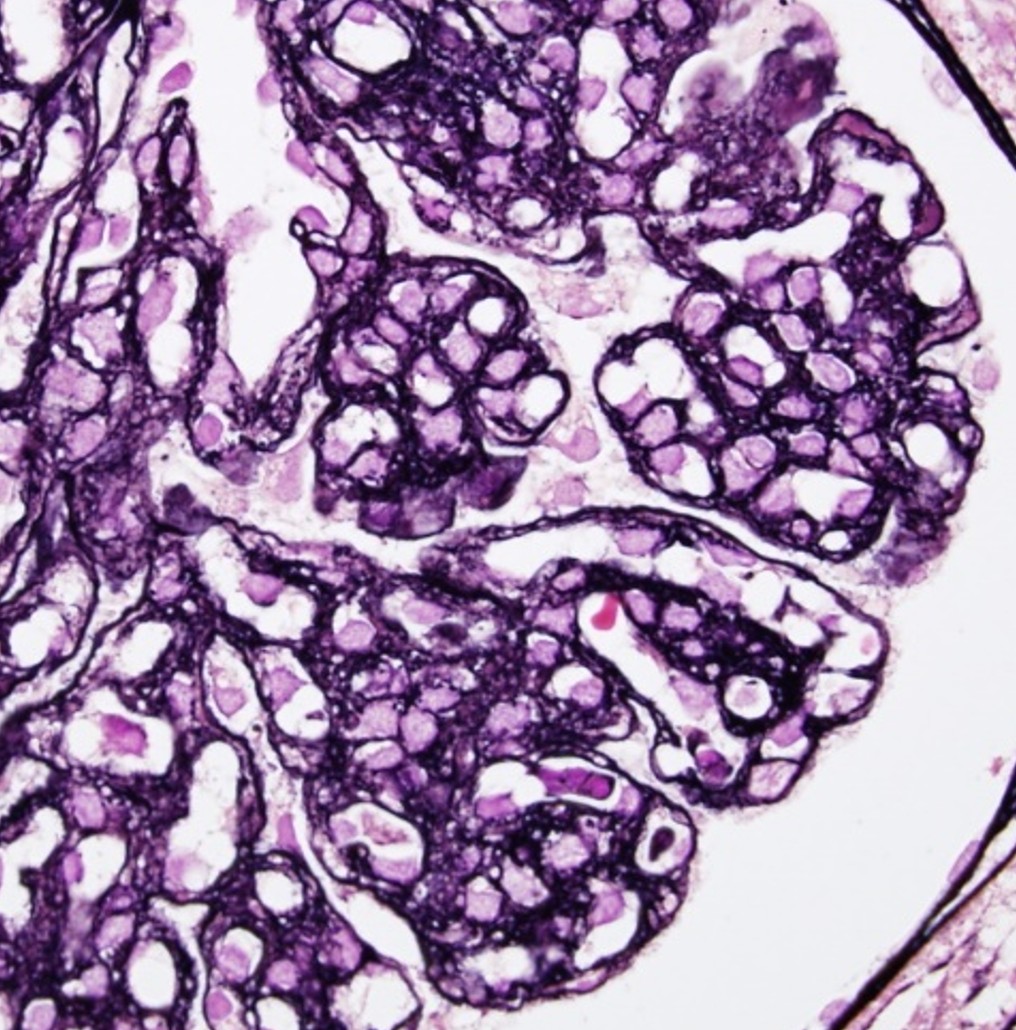
Fig1.jpg