Lecture Code : JS11-S4
Session Name : KSN-ISRNM-KSCN Joint Symposium
Session Topic : KSN-ISRNM-KSCN Joint Symposium
Date & Time, Place : June 13 (Sat) / 15:30-17:30 / Room 2 (GBR 102), 1F
Nutritional Support for Sarcopenia Prevention Among CKD Patients
Haelim Kim
Chungbuk National University Hospital, Republic of Korea
In March 2026, the Korea Disease Control and Prevention Agency’s National Institute of Health analyzed data from the Korea Cohort Study for Outcome in Patients With Chronic Kidney Disease (KNOW-CKD, Principal Investigator: Dr. Oh Guk-Hwan, Seoul National University Hospital). The study showed that muscle mass loss and protein-energy wasting (PEW) significantly affect kidney function decline and mortality in chronic kidney disease (CKD) patients.
After adjusting for age and comorbidities such as diabetes and hypertension, patients with the lowest muscle mass had a 4.47-fold higher risk of kidney function deterioration compared with those with the highest muscle mass. This indicates that sarcopenia in CKD is not merely age-related but a critical indicator linked to disease progression.
PEW was also associated with prognosis. Compared with patients meeting no PEW criteria, those meeting two or more criteria had a 2.78-fold higher mortality risk, and those meeting three or more criteria had a 3.78-fold increase. While traditional definitions use three criteria to predict mortality, this study showed that even two criteria are linked to higher mortality and cardiovascular complications. These findings underscore the need for early preventive interventions, including nutrition and exercise, to mitigate muscle loss.
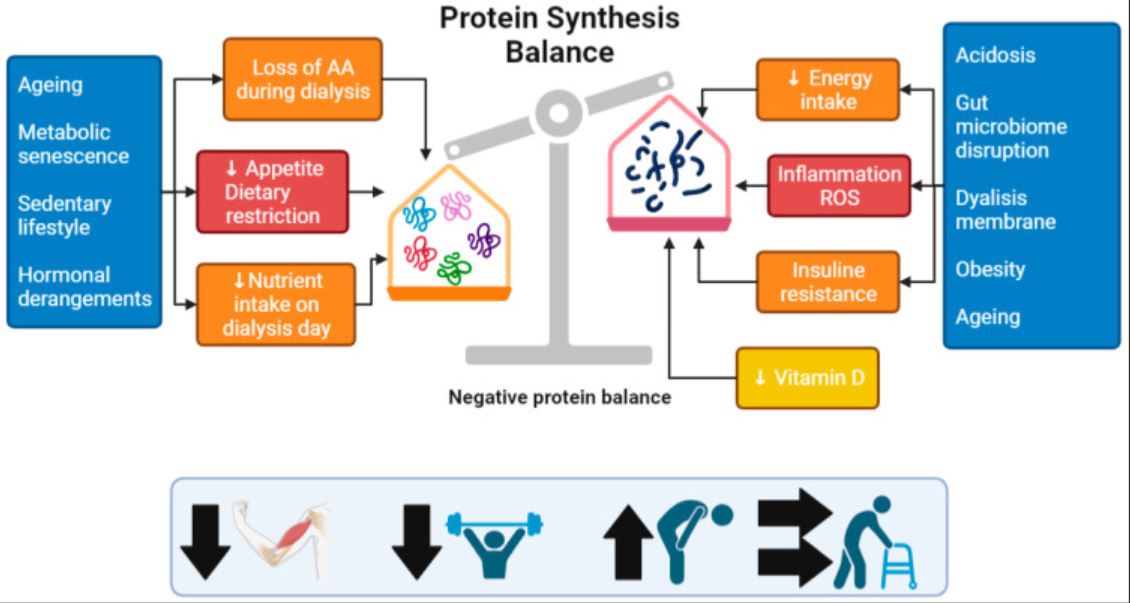
Mechanistically, sarcopenia arises when muscle protein breakdown exceeds synthesis, resulting in net protein loss. In CKD, chronic inflammation and uremic toxins accelerate protein degradation while suppressing synthesis, causing faster muscle loss than in healthy individuals. Other contributing factors include metabolic disturbances and comorbidities.
Therefore, nutritional management to prevent sarcopenia in CKD requires a balance between adequate protein provision and overall nutritional sufficiency. This includes very low-protein diets supplemented with essential amino acids and keto-analogues, plant-based proteins to reduce metabolic acidosis, high-bioavailability animal proteins, dietary patterns emphasizing low glycemic index and high fiber, omega-3 fatty acids, and sufficient caloric intake to spare protein.
Assessment of body composition should consider PEW risk factors, the limitations of published weight norms, and indices such as serum creatinine and cystatin C?based sarcopenia measures. Both oral and enteral nutrition should be individualized, accounting for energy and protein requirements, electrolyte disturbances, fluid restrictions, gastrointestinal status, and comorbidities.
In conclusion, this study highlights the importance of managing integrated dietary strategies that incorporate nutrition interventions to prevent muscle loss in CKD patients, combining functional assessment and body composition analysis for optimal clinical management.
Keywords: sarcopenia, Trends of nutrition requirements, nutrition assessment, enteral formula selection in CKD, Dietary pattern
table 1. Trends in Energy and Protein Requirements in Patients with Chronic Kidney Disease.JPG
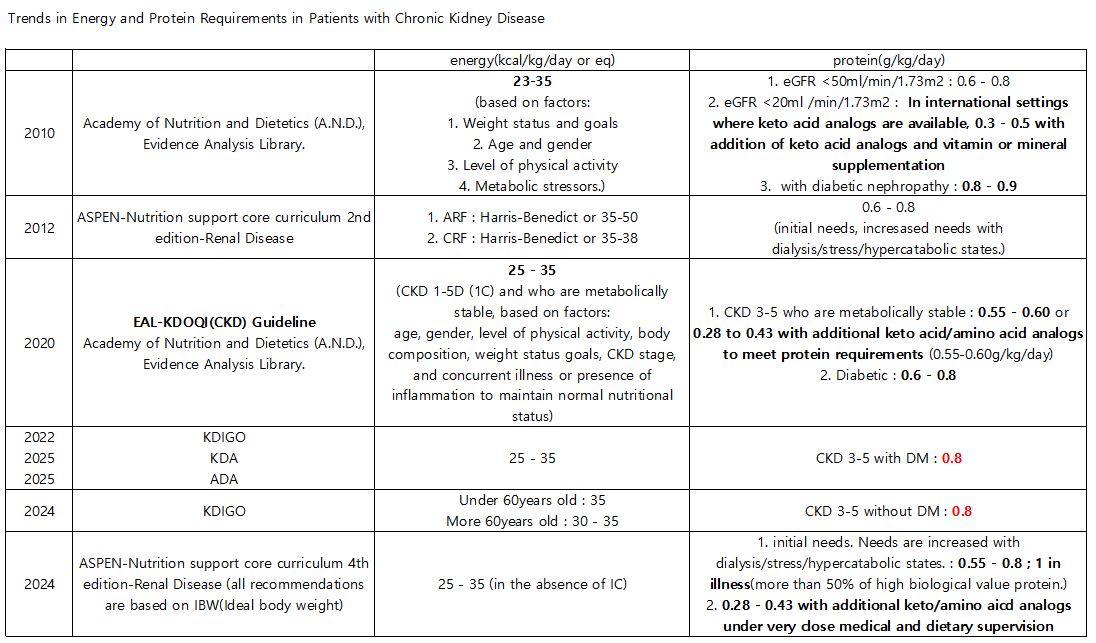
table 1. Trends in Energy and Protein Requirements in Patients with Chronic Kidney Disease.JPG