Abstract Type : Oral presentation
Abstract Submission No.: A-0988
Abstract Topic : Transplantation
Kidney Replacement Modality and Outcomes After De Novo Solid Cancer: Stage at Diagnosis, Treatment, and Survival in a Nationwide Cohort
Jeeyoung Kim1, Heajung Lee2, Subin Jeong3, Eunjeong Kang, Hajeong Lee
1Department of Internal Medicine-Nephrology, Chung-Ang University Hospital, Korea, Republic of
2Department of Department of Statistics and Data Science, Yonsei University, Korea, Republic of
3Department of Medical Research Institute, Seoul National University Hospital, Korea, Republic of
4Department of Transplantation Center, Seoul National University Hospital, Korea, Republic of
5Department of Internal Medicine, Seoul National University College of Medicine, Korea, Republic of
Objectives : Kidney transplant recipients (KTRs) and end-stage kidney disease (ESKD) patients face elevated cancer risk, but differences in stage at diagnosis and mortality remain unclear. We compared cancer stage at diagnosis and mortality among KTRs, ESKD patients, and the general population (GP) for stomach, colorectal, liver, and breast cancers.
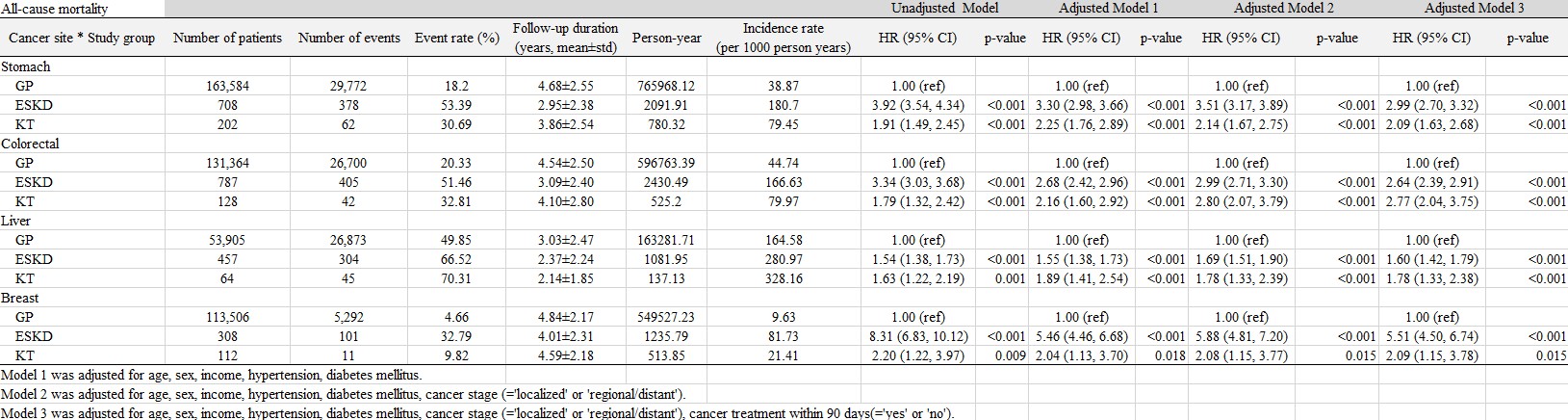
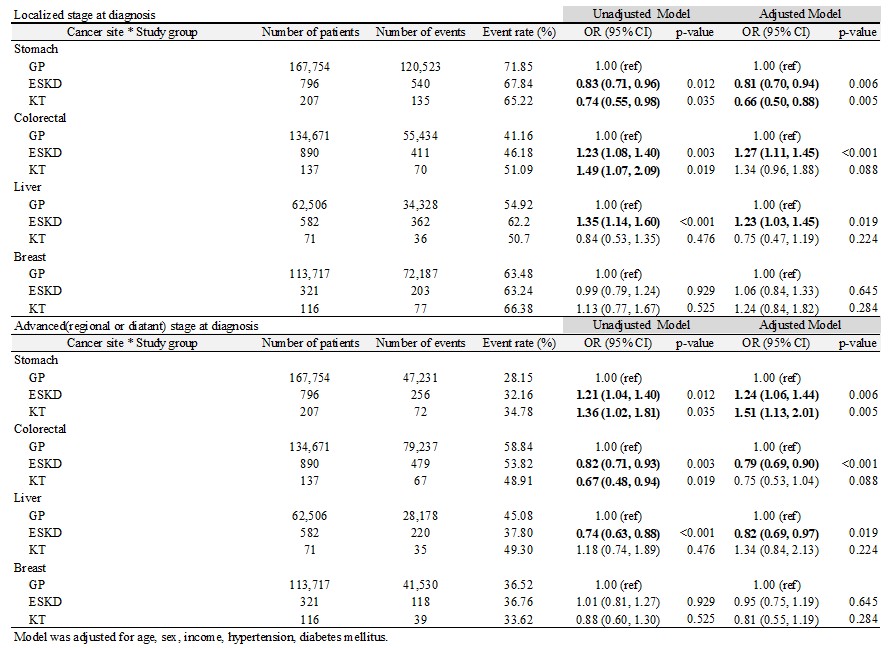
Methods : Using a nationwide Korean cancer registry linked to administrative claims data (2012–2019), we identified de-novo cancers among KTRs, ESKD patients on dialysis, and GP individuals. Cancer stage was classified using SEER summary staging. Logistic regression compared localized versus advanced-stage disease, and Cox models estimated hazard ratios (HRs) for mortality among patients surviving ≥90 days after diagnosis.
Results : We included 507,525 patients: 577 KTRs, 2,890 ESKD patients, and 504,058 GP individuals. KTRs were younger (58.7±9.6 years) than ESKD (66.5±10.8 years) and GP (61.3±12.1 years), and both groups had higher prevalence of hypertension and diabetes than GP. Compared with GP, KTRs with stomach cancer were less likely to present with localized disease (OR 0.66; 95% CI 0.50–0.88), and KTRs with liver cancer had lower odds of localized presentation versus ESKD (OR 0.56; 0.33–0.94). KTRs had higher all-cause mortality than GP for all sites: stomach HR 2.09 (1.63–2.68), colorectal HR 2.77 (2.04–3.75), liver HR 1.78 (1.33–2.38), and breast HR 2.09 (1.15–3.78). In KTR-versus-ESKD comparisons, KTRs had lower mortality for stomach (HR 0.65; 0.49–0.87) and breast cancer (HR 0.36; 0.19–0.70).
Conclusions : Both KTRs and ESKD patients had worse cancer outcomes than the GP, although KTRs showed a survival advantage over ESKD patients for certain cancers. More advanced stage at presentation for stomach and liver cancers in KTRs raises concern about current post-transplant surveillance, and supports development of cancer-site-specific strategies tailored separately for transplant recipients and dialysis patients.
Methods : Using a nationwide Korean cancer registry linked to administrative claims data (2012–2019), we identified de-novo cancers among KTRs, ESKD patients on dialysis, and GP individuals. Cancer stage was classified using SEER summary staging. Logistic regression compared localized versus advanced-stage disease, and Cox models estimated hazard ratios (HRs) for mortality among patients surviving ≥90 days after diagnosis.
Results : We included 507,525 patients: 577 KTRs, 2,890 ESKD patients, and 504,058 GP individuals. KTRs were younger (58.7±9.6 years) than ESKD (66.5±10.8 years) and GP (61.3±12.1 years), and both groups had higher prevalence of hypertension and diabetes than GP. Compared with GP, KTRs with stomach cancer were less likely to present with localized disease (OR 0.66; 95% CI 0.50–0.88), and KTRs with liver cancer had lower odds of localized presentation versus ESKD (OR 0.56; 0.33–0.94). KTRs had higher all-cause mortality than GP for all sites: stomach HR 2.09 (1.63–2.68), colorectal HR 2.77 (2.04–3.75), liver HR 1.78 (1.33–2.38), and breast HR 2.09 (1.15–3.78). In KTR-versus-ESKD comparisons, KTRs had lower mortality for stomach (HR 0.65; 0.49–0.87) and breast cancer (HR 0.36; 0.19–0.70).
Conclusions : Both KTRs and ESKD patients had worse cancer outcomes than the GP, although KTRs showed a survival advantage over ESKD patients for certain cancers. More advanced stage at presentation for stomach and liver cancers in KTRs raises concern about current post-transplant surveillance, and supports development of cancer-site-specific strategies tailored separately for transplant recipients and dialysis patients.
SOT_figure1.jpg
SOT_figure1.jpg