Abstract Type : Oral presentation
Abstract Submission No.: A-0947
Abstract Topic : Transplantation
Impact of Sex Mismatch in Spousal Kidney Transplantation: Loss of the Male-to-Female Advantage
Seunghyeok Choi1, Ji-Hyum Yeom1, Hyeong Wan Kim1, Sik Lee1, Byung Ha Chung2, Young Joo Kwon4, Yeon Ho Park5, Jaeseok Yang6, Myoung Soo Kim7, KOTRY Study group3
1Department of Internal Medicine-Nephrology, Chonbuk National University Hospital, Korea, Republic of
2Department of Internal Medicine-Nephrology, The Catholic University of Korea Seoul St. Mary's Hospital , Korea, Republic of
3Department of Study group, KOTRY, Korea, Republic of
4Department of Internal Medicine-Nephrology, Korea University Guro Hospital, Korea, Republic of
5Department of Surgery-Transplantation, Gachon University Gil Medical Center, Korea, Republic of
6Department of Internal Medicine-Nephrology, Yonsei University College of Medicine, Korea, Republic of
7Department of Surgery-Transplantation, Yonsei University College of Medicine, Korea, Republic of
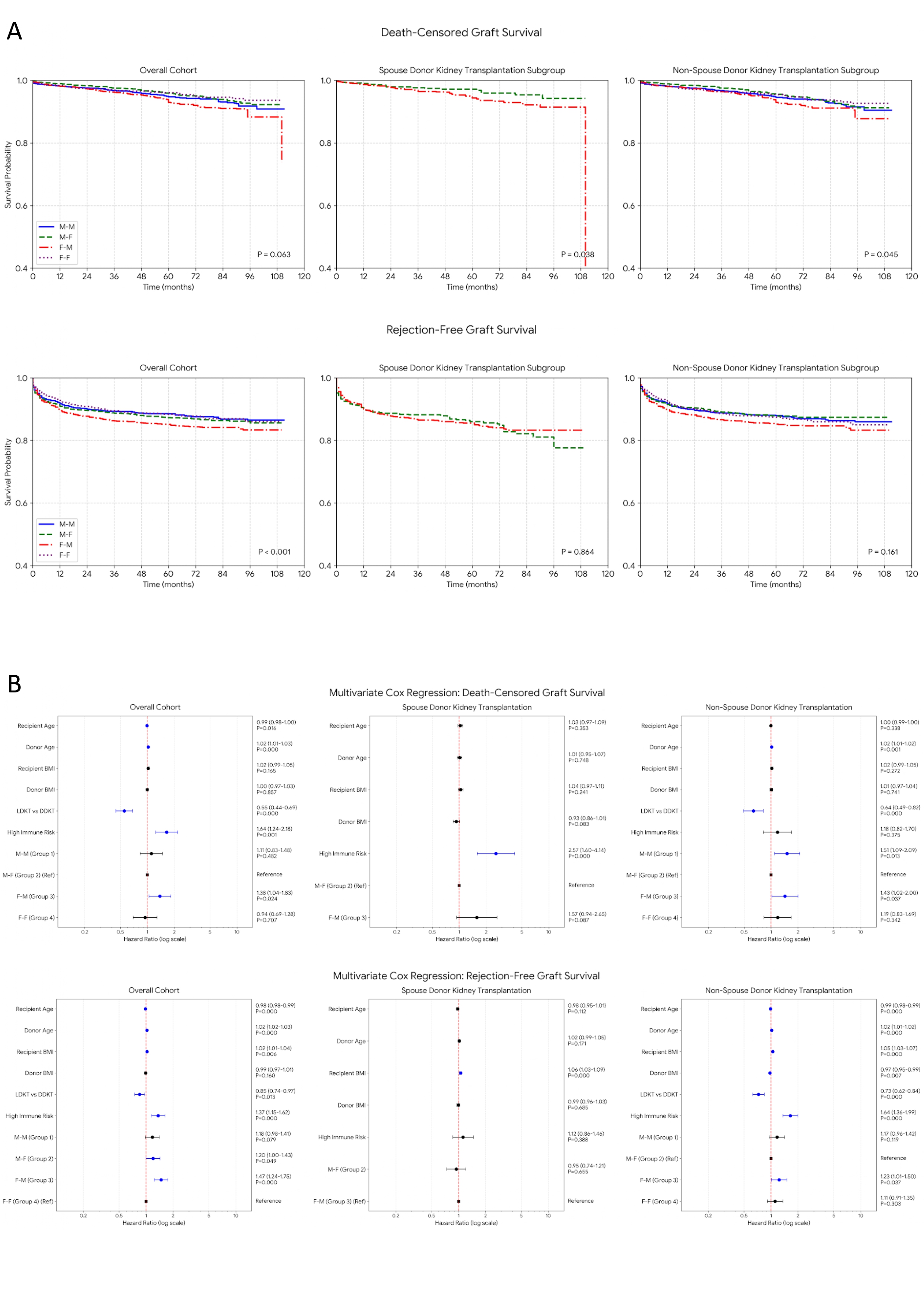
Methods : Using a KOTRY registry, we categorized recipients into four sex-mismatch groups (M-M, M-F, F-M, and F-F) and stratified them into non-SDKT and SDKT cohorts. Inverse probability of treatment weighting (IPTW) was applied to adjust for baseline differences. Clinical outcomes, including death-censored graft survival, rejection-free graft survival, incidence of rejection, and infection rates, were compared using weighted Cox regression and Chi-square tests.
Results : In the overall cohort, the F-M group had significantly higher risks of both graft failure (adjusted HR 1.43, P=0.037) and acute rejection (adjusted HR 1.23, P=0.037) compared to the M-F reference group, confirming the typical M-F advantage. In the SDKT cohort, the M-F group maintained its protective advantage in death-censored graft survival. However, this advantage was offset in terms of rejection-free survival (adjusted HR for F-M vs. M-F: 1.06, P=0.655). Furthermore, husband-to-wife (M-F) transplants in the SDKT group exhibited a significantly higher incidence of acute antibody-mediated rejection (AABMR) compared to wife-to-husband transplants (5.5% vs. 3.5%, P=0.003), along with a substantially higher 1-year infection rate (P<0.001).
Conclusions : In spousal kidney transplantation, the physiological advantage of a male donor's larger nephron mass is sufficient to preserve long-term death-censored graft survival. However, this benefit is completely offset in terms of rejection-free survival. This negation is driven by an immunological penalty—characterized by increased antibody-mediated rejections and subsequent infectious complications—which likely stems from unmeasured spousal sensitization, such as prior pregnancies. Consequently, husband-to-wife transplants require vigilant pre-transplant immunological screening and tailored post-transplant care.
KSN abstract figure_page-0001.jpg