Abstract Type : Oral presentation
Abstract Submission No.: A-0761
Abstract Topic : Interventional Nephrology
Multi-Organ POCUS Revealing High Flow Arteriovenous Fistula-Related Pulmonary Hypertension
Eun Jung Kim1, Kwangho Choi2, Hyunsuk Kim2, Hyungseok Lee3, DoHyoung Kim4
1Department of Internal Medicine-Nephrology, Dongtan Sacred Heart Hospital, Korea, Republic of
2Department of Internal Medicine-Nephrology, Chuncheon Sacred Heart Hospital, Korea, Republic of
3Department of Internal Medicine-Nephrology, Hallym University Sacred Heart Hospital, Korea, Republic of
4Department of Internal Medicine-Nephrology, Kangnam Sacred Heart Hospital, Korea, Republic of
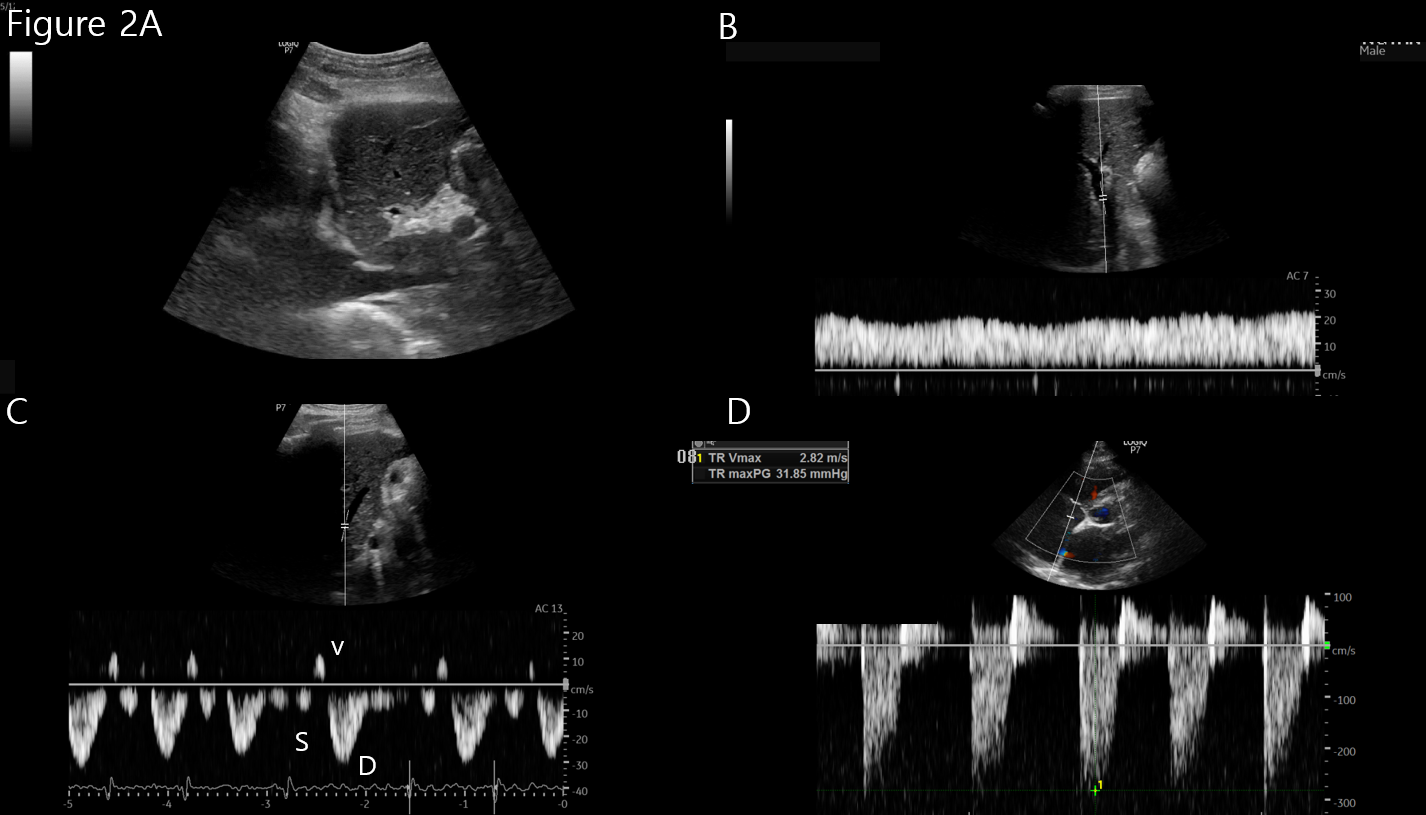
Case Study : A 58-year-old man with diabetic end-stage renal disease on maintenance hemodialysis since 2019 was referred for worsening pulmonary hypertension. He had a left brachiocephalic arteriovenous fistula (AVF) created in 2019 and a right brachiocephalic AVF created in 2021 due to recurrent thrombosis, resulting in functioning AVFs in both arms. Access flow assessment showed brachial artery blood flow rates of 450 mL/min in the left AVF and 920 mL/min in the right AVF. Multi-organ point-of-care ultrasound (POCUS) was performed to evaluate hemodynamic status. Lung ultrasound demonstrated bilateral multiple B-lines with pleural effusions. The inferior vena cava diameter was 2.3 cm with reduced collapsibility. Doppler evaluation revealed a portal vein pulsatility fraction greater than 50% and systolic flow reversal in the hepatic vein waveform, indicating significant venous congestion. Focused cardiac ultrasound demonstrated right and left atrial enlargement with mitral regurgitation. The E/e′ ratio was 23.5. Tricuspid regurgitation was observed in a modified apical four-chamber view with a TRVmax of 4.6 m/s, corresponding to an estimated right ventricular systolic pressure above 60 mmHg, consistent with severe pulmonary hypertension(Figure1). Cardiac output was estimated at 2.99 L/min, while total access flow was approximately 1,370 mL/min, resulting in Qa/CO >0.3, suggesting a high-flow AVF–related hemodynamic burden. The patient subsequently underwent AVF ligation and aggressive volume optimization with bilateral pleural drainage and removal of 7 kg of fluid. Follow-up multi-organ POCUS demonstrated improvement in venous congestion, including normalization of the portal vein waveform, improvement of hepatic vein Doppler patterns, and reduction of TRVmax to 2.8 m/s with E/e′ decreasing to 15, indicating improvement in pulmonary hypertension(Figure2). This case illustrates that multi-organ POCUS can identify venous congestion and high-flow AVF–related hemodynamic burden, guide therapeutic decisions such as AVF ligation and volume optimization, and allow real-time assessment of hemodynamic improvement in patients with pulmonary hypertension.
Figure 1 ..png
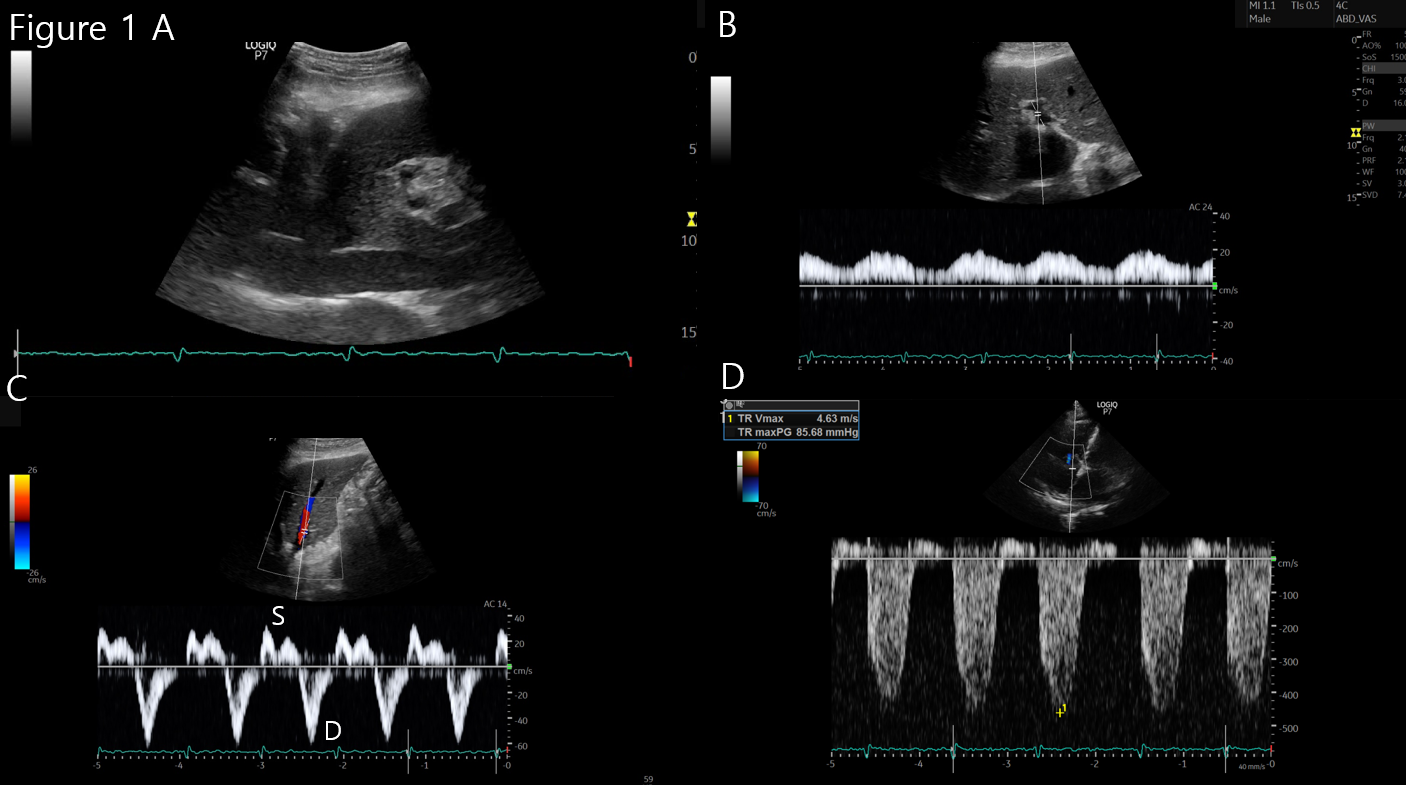
Figure 1 ..png