
Abstract Type : Oral presentation
Abstract Submission No.: A-0730
Abstract Topic : Acute Kidney Injury
Long-term Kidney Outcomes After Immune Checkpoint Inhibitor Therapy Compared with Conventional Chemotherapy
Inyong Jeong1, Jeonghwan Kim3, Gang-Jee Ko2, Ho-Jin Lee4, Myung-Gyu Kim4, Sang-Kyung Jo4, Hwamin Lee4, Se Won Oh4
1Department of Department of Biomedical Informatics, Korea University College of Medicine, Seoul, Republic of Korea, Korea, Republic of
2Department of Otorhinolaryngology, Korea University Ansan Hospital, Korea, Republic of
3Department of Internal Medicine-Nephrology, Korea University Guro Hospital, Korea, Republic of
4Department of Internal Medicine-Nephrology, Korea University Anam Hospita, Korea, Republic of
Objectives : Immune checkpoint inhibitors (ICIs) have become a standard therapy for various cancers. Although ICIs improve survival, they may cause immune-related adverse events, including acute kidney injury. However, their long-term renal outcomes compared with conventional chemotherapy remain unclear.
Methods : Data were obtained from the electronic health records of two tertiary referral centers (2015–2024). Among 19,668 patients initiating first-line systemic anticancer therapy, propensity score matching on 12 covariates was performed, yielding a matched cohort (N=2,172; 1,086 pairs).
Results : In the matched cohort, the mean age was 65.5 years, 70.8% were male, and the mean baseline eGFR was 93.3 mL/min/1.73 m²; The median follow-up was 11.1 months (IQR 4.7–21.0) in the ICI group and 10.4 months (IQR 4.7–22.2) in the non-ICI group. The ICI group experienced a significant early decline within the first 6 months (Δslope −0.352 mL/min/1.73 m²/month, p<0.001), followed by a significant attenuation in the rate of decline during months 6–12 (Δslope +0.227, p=0.002), after which no between-group difference remained (Δslope +0.028, p=0.22). The risk of ≥30% eGFR decline showed a statistically significant but modest association with ICI therapy (HR 1.16, 95% CI 1.02–1.31, p=0.019), which was attenuated after competing risk adjustment. In contrast, de novo overt proteinuria was consistently associated with ICI: stratified Cox HR 1.84 (95% CI 1.37–2.47, p<0.001). Subgroup analysis by ICI class revealed that anti-PD-1 therapy was associated with both eGFR decline and proteinuria, whereas anti-PD-L1 therapy showed no eGFR decline but a markedly elevated risk of proteinuria (HR 3.12, 95% CI 1.66–5.89, p<0.001). All-cause mortality was higher in the ICI group (HR 1.49, 95% CI 1.30–1.70, p<0.001).
Conclusions : ICI therapy was associated with an early decline in eGFR followed by partial recovery and an increased risk of proteinuria.
Methods : Data were obtained from the electronic health records of two tertiary referral centers (2015–2024). Among 19,668 patients initiating first-line systemic anticancer therapy, propensity score matching on 12 covariates was performed, yielding a matched cohort (N=2,172; 1,086 pairs).
Results : In the matched cohort, the mean age was 65.5 years, 70.8% were male, and the mean baseline eGFR was 93.3 mL/min/1.73 m²; The median follow-up was 11.1 months (IQR 4.7–21.0) in the ICI group and 10.4 months (IQR 4.7–22.2) in the non-ICI group. The ICI group experienced a significant early decline within the first 6 months (Δslope −0.352 mL/min/1.73 m²/month, p<0.001), followed by a significant attenuation in the rate of decline during months 6–12 (Δslope +0.227, p=0.002), after which no between-group difference remained (Δslope +0.028, p=0.22). The risk of ≥30% eGFR decline showed a statistically significant but modest association with ICI therapy (HR 1.16, 95% CI 1.02–1.31, p=0.019), which was attenuated after competing risk adjustment. In contrast, de novo overt proteinuria was consistently associated with ICI: stratified Cox HR 1.84 (95% CI 1.37–2.47, p<0.001). Subgroup analysis by ICI class revealed that anti-PD-1 therapy was associated with both eGFR decline and proteinuria, whereas anti-PD-L1 therapy showed no eGFR decline but a markedly elevated risk of proteinuria (HR 3.12, 95% CI 1.66–5.89, p<0.001). All-cause mortality was higher in the ICI group (HR 1.49, 95% CI 1.30–1.70, p<0.001).
Conclusions : ICI therapy was associated with an early decline in eGFR followed by partial recovery and an increased risk of proteinuria.
figure1_ICI.jpg
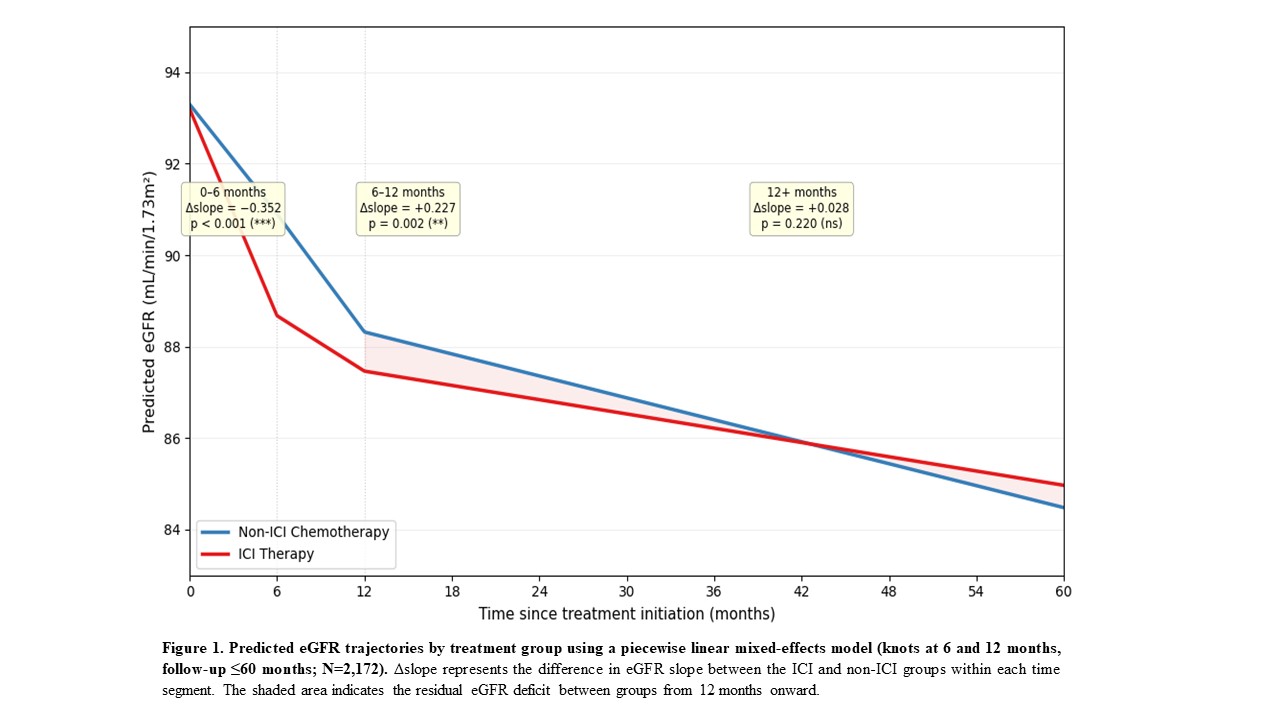
figure1_ICI.jpg
