Abstract Type : Oral presentation
Abstract Submission No.: A-0658
Abstract Topic : Non-dialysis CKD
Association between Skeletal Muscle Mass and Clinical Outcomes of Chronic Kidney Disease
MISO HA1, Jiyun Jung5, Jiin Park4, Yong Chul Kim2, Jae Yoon Park3
1Department of Internal Medicine, Seoul National University Hospital, Korea, Republic of
2Department of Internal Medicine-Nephrology, Seoul National University Hospital, Korea, Republic of
3Department of Internal Medicine-Nephrology, Dongguk University Ilsan Hospital, Korea, Republic of
4Department of Internal Medicine-Nephrology, Kangwon National University Hospital, Korea, Republic of
5Department of Biostatistics, Dongguk University Ilsan Hospital, Korea, Republic of
Objectives : Sarcopenia is highly prevalent among patients with chronic kidney disease (CKD) and may contribute to the elevated risk of adverse clinical outcomes in this population. However, large-scale evidence examining the relationship between objectively quantified muscle mass and cardiorenal outcomes remains scarce. Therefore, we leveraged a large CKD cohort to quantify muscle mass and evaluate its associations with cardiorenal and mortality outcomes.
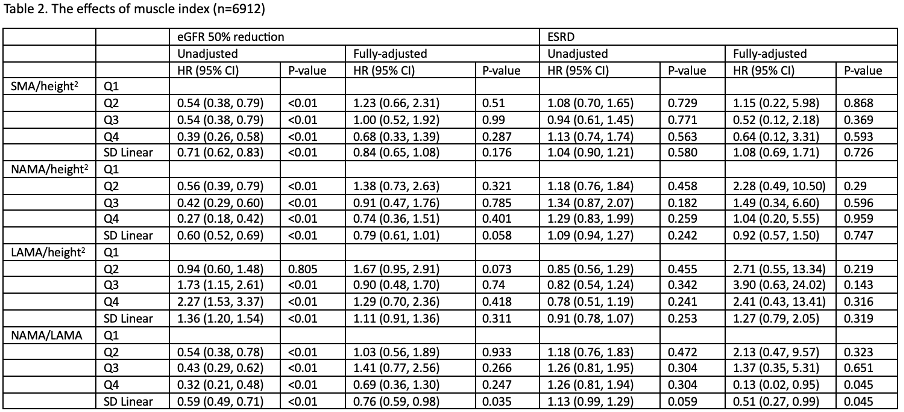
Methods : We conducted a retrospective cohort study of 10,125 adults with CKD who underwent abdominal computed tomography at Seoul National University Hospital between 2001 and 2023. Patients with end-stage malignancy at the time of CKD diagnosis were excluded. Skeletal muscle area (SMA) and muscle quality (NAMA, LAMA) were quantified at the L3 vertebral level using CT imaging. Outcomes included all-cause mortality, major adverse cardiovascular events (MACE), ≥50% decline in eGFR, and progression to end-stage renal disease (ESRD). Associations were evaluated using multivariable Cox proportional hazards models adjusted for demographic and clinical covariates.
Results : During a median follow-up of 8 years, Greater SMA/height² and NAMA/LAMA were independently associated with lower risks of all-cause mortality (adjusted HR 0.78 [95% CI 0.63–0.97] and 0.75 [0.60–0.93], respectively). Greater NAMA/LAMA was also associated with reduced risks of MACE (adjusted HR 0.62 [0.45–0.86]), ≥50% eGFR decline (adjusted HR 0.76 [0.59–0.98]), and progression to ESRD (adjusted HR 0.51 [0.27–0.99]).
Conclusions : Greater muscle mass and better muscle quality were associated with lower risks of All-cause mortality, eGFR decline, and MACE incidence in CKD patients. In patients with CKD, CT-derived skeletal muscle assessment is a stronger biomarker than body weight or body mass index alone. Notably, Our results suggest that muscle quality may serve as potential risk stratification tool for Cardiorenal outcomes in the future management of CKD.
Methods : We conducted a retrospective cohort study of 10,125 adults with CKD who underwent abdominal computed tomography at Seoul National University Hospital between 2001 and 2023. Patients with end-stage malignancy at the time of CKD diagnosis were excluded. Skeletal muscle area (SMA) and muscle quality (NAMA, LAMA) were quantified at the L3 vertebral level using CT imaging. Outcomes included all-cause mortality, major adverse cardiovascular events (MACE), ≥50% decline in eGFR, and progression to end-stage renal disease (ESRD). Associations were evaluated using multivariable Cox proportional hazards models adjusted for demographic and clinical covariates.
Results : During a median follow-up of 8 years, Greater SMA/height² and NAMA/LAMA were independently associated with lower risks of all-cause mortality (adjusted HR 0.78 [95% CI 0.63–0.97] and 0.75 [0.60–0.93], respectively). Greater NAMA/LAMA was also associated with reduced risks of MACE (adjusted HR 0.62 [0.45–0.86]), ≥50% eGFR decline (adjusted HR 0.76 [0.59–0.98]), and progression to ESRD (adjusted HR 0.51 [0.27–0.99]).
Conclusions : Greater muscle mass and better muscle quality were associated with lower risks of All-cause mortality, eGFR decline, and MACE incidence in CKD patients. In patients with CKD, CT-derived skeletal muscle assessment is a stronger biomarker than body weight or body mass index alone. Notably, Our results suggest that muscle quality may serve as potential risk stratification tool for Cardiorenal outcomes in the future management of CKD.
table1.png
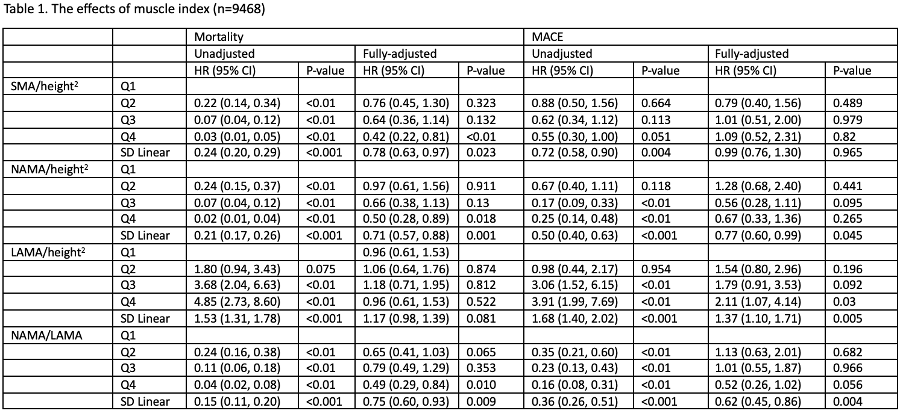
table1.png