Abstract Type : Oral presentation
Abstract Submission No.: A-0450
Abstract Topic : Acute Kidney Injury
Development of a Mode-Change-Based Strategy for Discontinuation During Ongoing CKRT (DECISION-CKRT): A Multicenter Prospective Observational Study
Yohan Park1, Sua Lee3, Jieun Shin2, Ji Won Lee1, Haeun Lee4, Hae Ri Kim5, Soyoung Lee5, Harin Rhee6
1Department of Internal Medicine-Nephrology, Konyang University Hospital, Korea, Republic of
2Department of Biomedical Informatics, Konyang University, Korea, Republic of
3Department of Internal Medicine-Nephrology, Kangnam Sacred Heart Hospital, Korea, Republic of
4Department of Internal Medicine-Nephrology, Presbyterian Medical Center, Korea, Republic of
5Department of Internal Medicine-Nephrology, Chungnam National University Sejong Hospital, Korea, Republic of
6Department of Internal Medicine-Nephrology, Pusan National University Hospital, Korea, Republic of
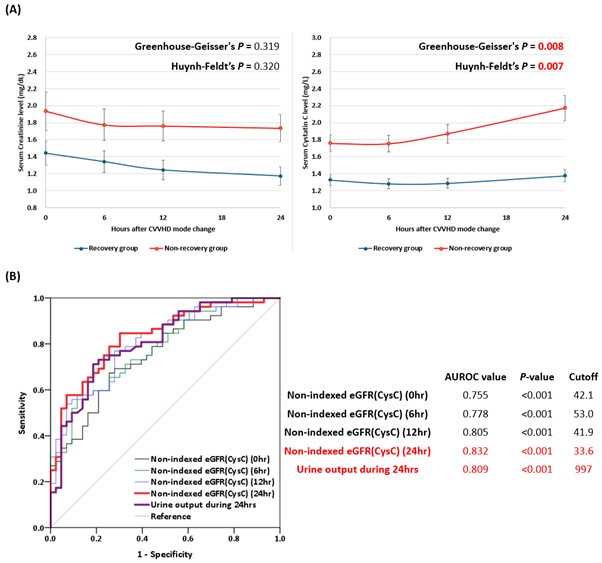
Methods : In this multicenter prospective observational study, CKRT modality was switched from continuous veno-venous hemodiafiltration (CVVHDF) to continuous veno-venous hemodialysis (CVVHD). Serum creatinine and cystatin C (CysC) were measured at 0, 6, 12, and 24 hours after the mode change, and urine output was measured over the same 24-hour period. After completion of the 24-hour sampling, CKRT was discontinued. Kidney recovery was defined as the absence of KRT re-initiation within 7 days after discontinuation. Receiver operating characteristic (ROC) analysis was performed to identify predictors of kidney recovery.
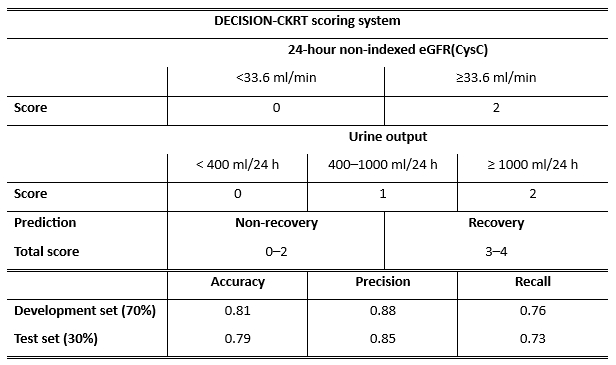
Results : Among the 95 patients, 52 achieved kidney recovery and 43 required KRT re-initiation. Among evaluated parameters, eGFR(CysC) at 24 hours after the mode change showed the best performance for predicting kidney recovery (AUROC 0.832), with an optimal cutoff value of 33.6 ml/min (Figure 1). Based on these findings, a scoring system combining urine output and eGFR(CysC) was developed. One point was assigned for urine output ≥400 mL/24 h, two points for urine output ≥1000 mL/24 h, and two points for eGFR(CysC) ≥33.6 ml/min at 24 hours, yielding a total score of 0–4. The model achieved accuracy of 0.81 in the development set and 0.79 in the test set, showing consistent accuracy across datasets (Table 1).
Conclusions : We developed the DECISION-CKRT scoring system, a novel protocolized strategy enabling assessment of kidney recovery through a simple mode-switch approach during ongoing CKRT. By combining eGFR(CysC) kinetics with urine output during the 24-hour evaluation period, this approach allows clinicians to determine kidney recovery without stopping CKRT. This reproducible and practical protocol provides a framework for CKRT discontinuation.
Figure_1.jpg
Figure_1.jpg