Abstract Type : Oral presentation
Abstract Submission No.: A-0331
Abstract Topic : Big Data
External Validation And Recalibration Of International Prognostic Models For Chronic Kidney Disease In The KNOW-CKD
Sangjun Lee1, Minsang Kim4, Hajeong Lee4, Sue K. Park1, Kook-Hwan Oh4
1Department of Preventive Medicine, Seoul National University College of Medicine, Korea, Republic of
2Department of Cancer Research Institute, Seoul National University, Korea, Republic of
3Department of Genomic Medicine Institute, Medical Research Center, Seoul National University, Korea, Republic of
4Department of Internal Medicine, Seoul National University Hospital, Korea, Republic of
Objectives : To evaluate the transportability of the Kidney Failure Risk Equation and KDPredict in the Korean KNOW-CKD cohort and to develop locally refitted models for kidney failure, all-cause mortality, and composite outcomes.
Methods : Adults enrolled in phases 1 and 2 of KNOW-CKD were analyzed. After excluding participants with missing outcomes or predictors, baseline estimated glomerular filtration rate below 15 mL/min/1.73 m2, polycystic kidney disease, or missing proteinuria data, 2,871 participants remained. Cox models mirrored the original 4-variable and 8-variable Kidney Failure Risk Equation and 4-variable and 6-variable KDPredict structures. External validation used published coefficients with baseline hazard re-estimated in KNOW-CKD for absolute-risk recalibration. Internal refit models re-estimated coefficients in KNOW-CKD. Performance was assessed using time-dependent area under the curve at 2, 5, and 10 years.
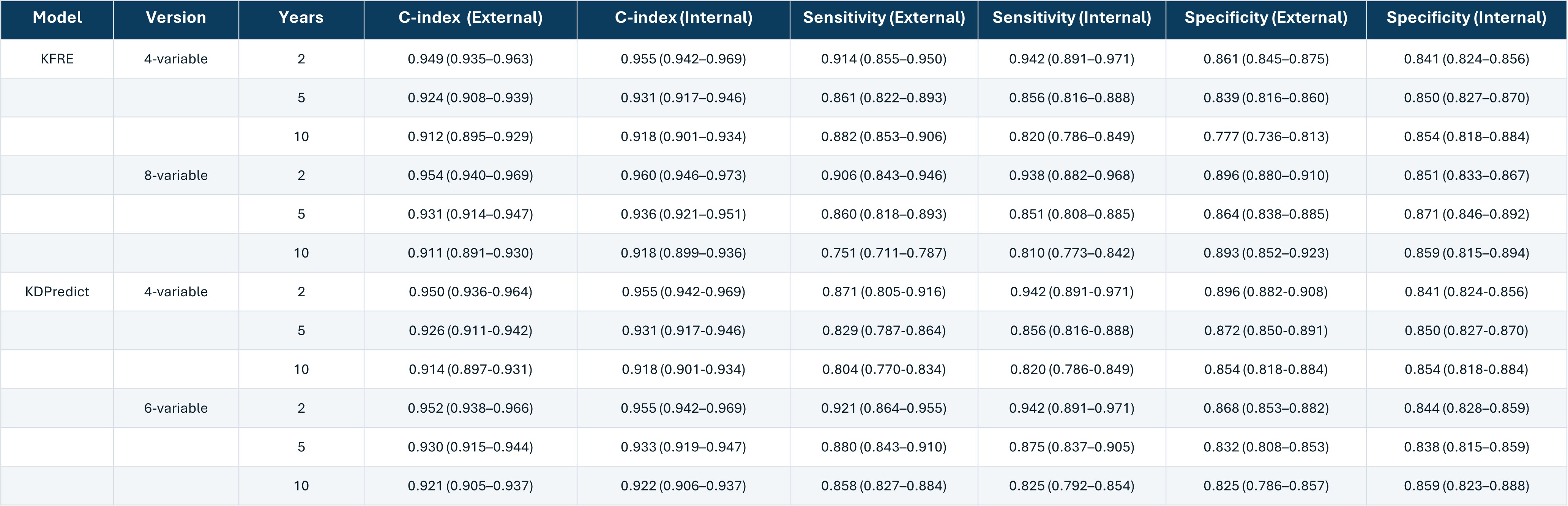
Results : For kidney failure, external models showed excellent discrimination, with time-dependent area under the curve values of 0.911-0.954 for Kidney Failure Risk Equation models and 0.914-0.952 for KDPredict models; internally refit models showed similar performance, ranging from 0.918-0.960 and 0.918-0.955, respectively. For all-cause mortality, external discrimination was modest, ranging from 0.650-0.778, but improved after refitting in KNOW-CKD to 0.796-0.834. Composite outcome performance was moderate to strong externally, ranging from 0.723-0.886, and improved further after refitting to 0.780-0.892. Risk-factor directions were largely preserved for kidney failure, whereas coefficient magnitudes differed more substantially for mortality and composite outcomes.
Conclusions : International kidney failure models generalized well to Korean patients with chronic kidney disease, whereas mortality and composite outcome prediction required local refitting and recalibration. These findings support population-specific implementation and provide the basis for a Korean absolute-risk prediction tool.
Methods : Adults enrolled in phases 1 and 2 of KNOW-CKD were analyzed. After excluding participants with missing outcomes or predictors, baseline estimated glomerular filtration rate below 15 mL/min/1.73 m2, polycystic kidney disease, or missing proteinuria data, 2,871 participants remained. Cox models mirrored the original 4-variable and 8-variable Kidney Failure Risk Equation and 4-variable and 6-variable KDPredict structures. External validation used published coefficients with baseline hazard re-estimated in KNOW-CKD for absolute-risk recalibration. Internal refit models re-estimated coefficients in KNOW-CKD. Performance was assessed using time-dependent area under the curve at 2, 5, and 10 years.
Results : For kidney failure, external models showed excellent discrimination, with time-dependent area under the curve values of 0.911-0.954 for Kidney Failure Risk Equation models and 0.914-0.952 for KDPredict models; internally refit models showed similar performance, ranging from 0.918-0.960 and 0.918-0.955, respectively. For all-cause mortality, external discrimination was modest, ranging from 0.650-0.778, but improved after refitting in KNOW-CKD to 0.796-0.834. Composite outcome performance was moderate to strong externally, ranging from 0.723-0.886, and improved further after refitting to 0.780-0.892. Risk-factor directions were largely preserved for kidney failure, whereas coefficient magnitudes differed more substantially for mortality and composite outcomes.
Conclusions : International kidney failure models generalized well to Korean patients with chronic kidney disease, whereas mortality and composite outcome prediction required local refitting and recalibration. These findings support population-specific implementation and provide the basis for a Korean absolute-risk prediction tool.
Figure1.jpg
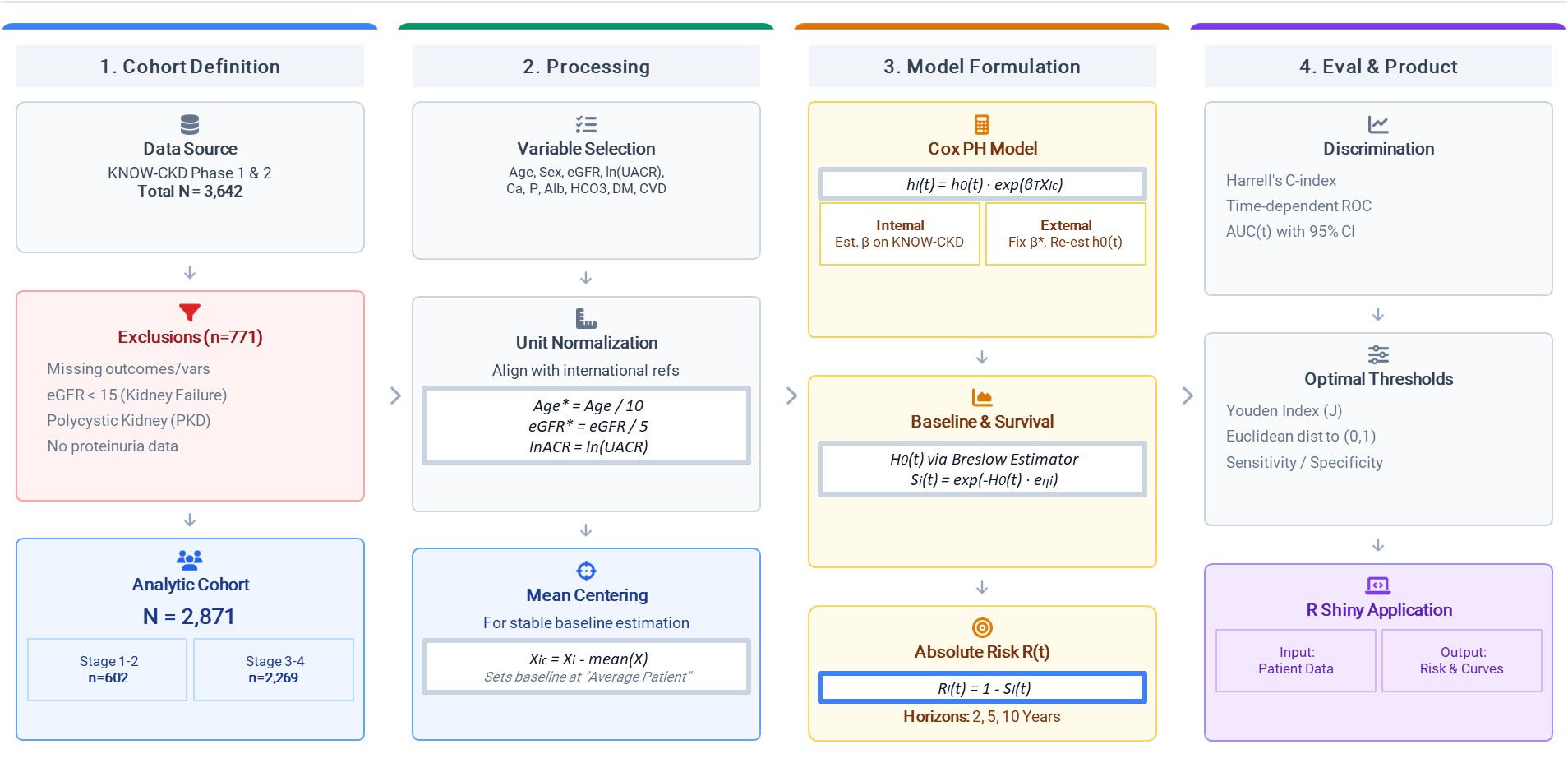
Figure1.jpg