Abstract Type : Oral presentation
Abstract Submission No.: A-0286
Abstract Topic : Glomerular and Tubulointerstitial Disorders
Distinct Associations of Histologic Activity and Chronicity with Short- and Long-Term Renal Outcomes in Lupus Nephritis
Hyeran Park1, Ji-Won Min2, Yu Ah Hong3, Seok Joon Shin6, Sungjin Chung4, Young Soo Kim7, Hyung Wook Kim1, Byung Soo Kim5, Cheol Whee Park1, Yong Kyun Kim1
1Department of Internal Medicine-Nephrology, The Catholic University of Korea St. Vincent's Hospital , Korea, Republic of
2Department of Internal Medicine-Nephrology, The Catholic University of Korea Bucheon St. Mary's Hospital , Korea, Republic of
3Department of Internal Medicine-Nephrology, The Catholic University of Korea Daejeon St. Mary's Hospital , Korea, Republic of
4Department of Internal Medicine-Nephrology, The Catholic University of Korea Yeouido St. Mary's Hospital , Korea, Republic of
5Department of Internal Medicine-Nephrology, The Catholic University of Korea Eunpyeong St. Mary's Hospital, Korea, Republic of
6Department of Internal Medicine-Nephrology, Incheon St. Mary's hospital, The Catholic University of Korea, Korea, Republic of
7Department of Internal Medicine-Nephrology, The Catholic University of Korea Uijeongbu St. Mary's Hospital , Korea, Republic of
Methods : We conducted a retrospective cohort study of patients with biopsy-proven LN. Baseline kidney biopsies were scored using AI and CI according to standard criteria. The primary outcomes were the 5-year composite renal outcome (≥40% decline in estimated glomerular filtration rate (eGFR) or progression to end-stage kidney disease) and 12-month change in eGFR. Secondary outcomes included treatment response at 6 and 12 months, categorized as treatment failure (TF), partial response (PR), or complete response (CR). Associations were evaluated using multivariable regression models adjusted for clinical covariates and Kaplan–Meier survival analyses.
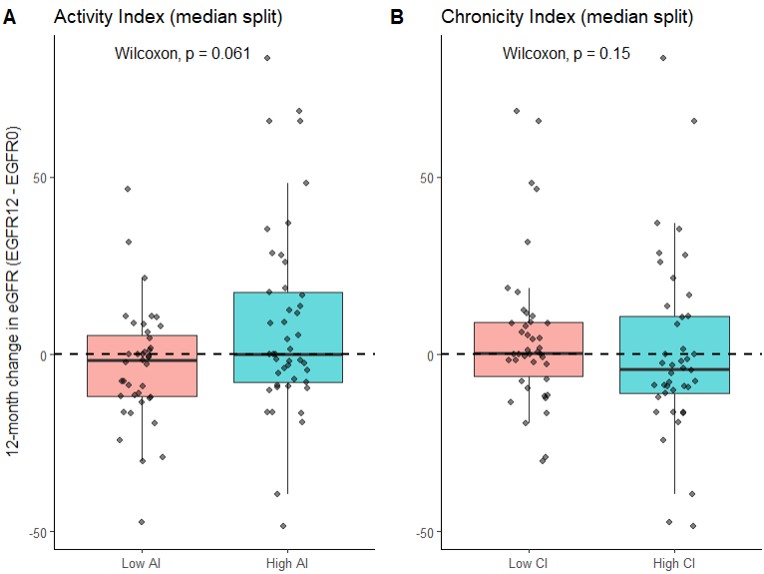
Results : A total of 116 patients were included, with a median follow-up of 4.9 years. In multivariable logistic regression adjusted for age and baseline proteinuria, CI independently predicted the 5-year composite renal outcome (OR 1.029; 95% CI 1.008–1.051; p = 0.02), whereas AI was not associated with long-term outcomes. Patients with higher CI had significantly poorer renal event-free survival (Figure 1, log-rank p = 0.025). In contrast, higher AI scores were independently associated with 12-month change in eGFR (β = 0.392 per point increase; 95% CI 0.02–0.76; p = 0.038), while CI showed no significant association with short-term renal functional change. In median-split analyses, higher AI demonstrated a trend toward greater 12-month eGFR change (Figure 2, Wilcoxon p = 0.061), whereas no significant differences were observed between CI groups. Neither AI nor CI was significantly associated with treatment response at 6 or 12 months.
Conclusions : CI predicted long-term renal outcomes, whereas AI was associated with short-term renal functional changes; neither predicted early treatment response.
Figure1_KSN.jpg
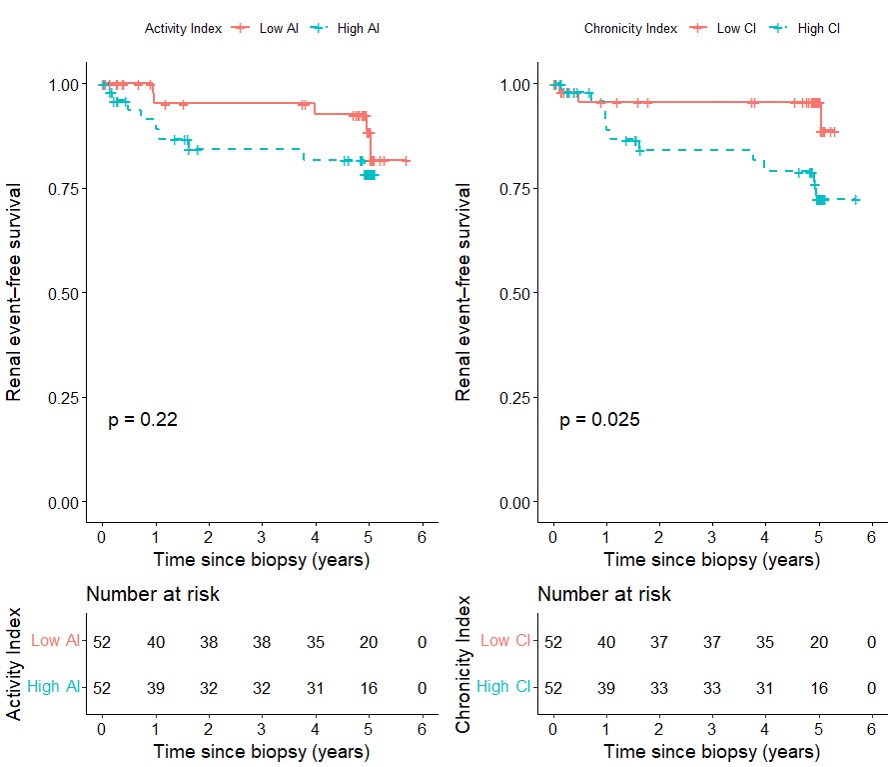
Figure1_KSN.jpg