Abstract Type : Oral presentation
Abstract Submission No.: A-0237
Abstract Topic : Interventional Nephrology
Central Venous Catheter as Permanent Vascular Access Should Be Avoided Even in the Oldest-Old Population Undergoing Dialysis: A Nationwide Cohort Study
JooUn Park1, Min-ho Kim2, Chang MIn Park3, Hanbi Lee1, Yaeni Kim1, Hye Eun Yoon1, Byung Ha Chung1, Cheol Whee Park1, Seok Joon Shin4, Hoon Suk Park1
1Department of Internal Medicine-Nephrology, The Catholic University of Korea Seoul St. Mary's Hospital , Korea, Republic of
2Department of Ewha Medical Data Organization, Ewha Womans University Medical Center, Korea, Republic of
3Department of Internal Medicine-Nephrology, The Catholic University of Korea Uijeongbu St. Mary's Hospital , Korea, Republic of
4Department of Internal Medicine-Nephrology, Incheon St. Mary's hospital, The Catholic University of Korea, Korea, Republic of
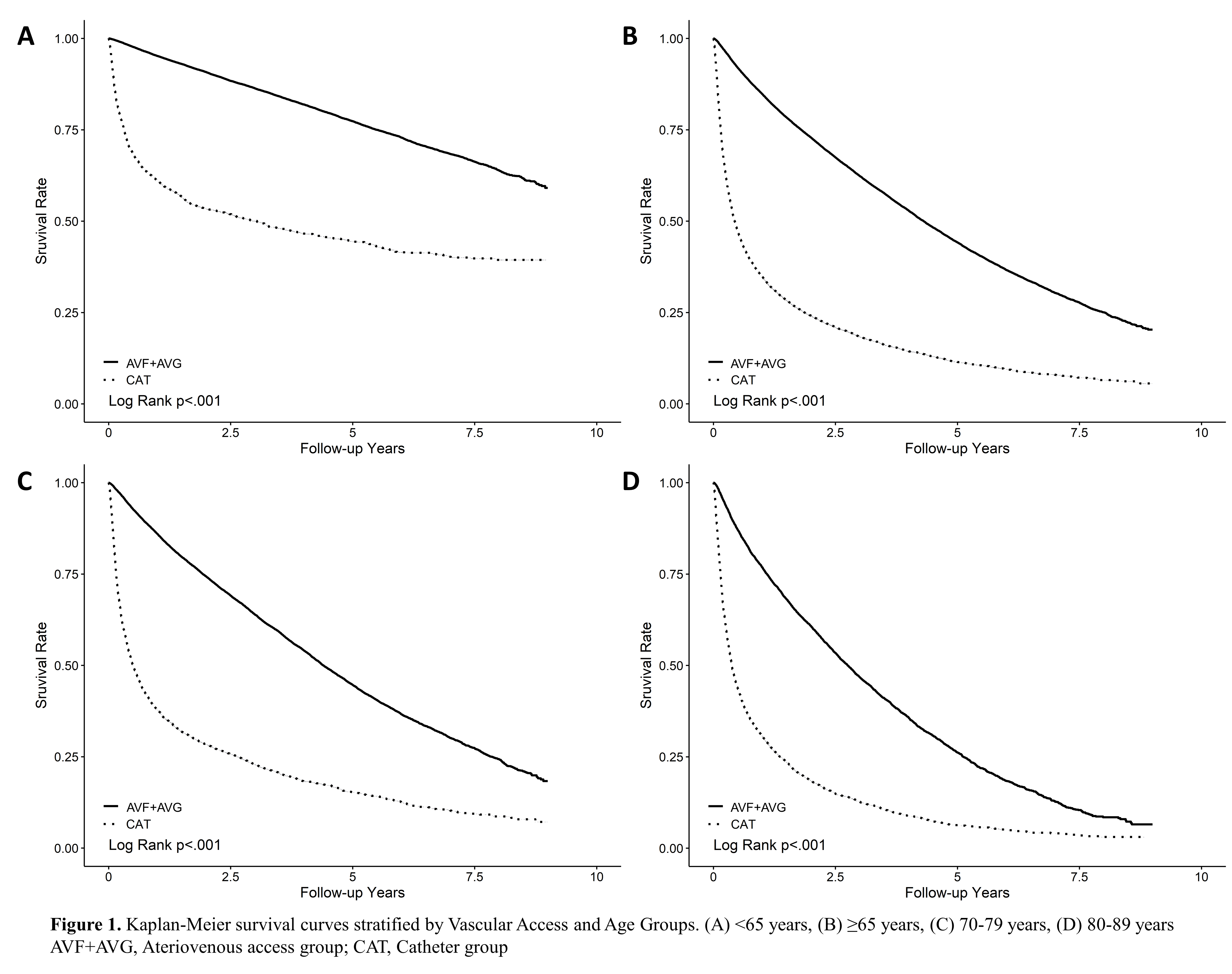
Methods : This nationwide retrospective cohort study included 79,286 adult patients (≥18 years) who initiated maintenance hemodialysis between 2012 and 2021, identified from the Korean National Health Insurance Service (NHIS) database. Patients were categorized as follows by permanent vascular access type: AV fistula (AVF), AV graft (AVG), or CVC. The primary outcome evaluated was all-cause mortality. Kaplan–Meier survival analysis and Cox proportional hazards models were used to assess mortality across vascular access types. Analyses were stratified by age group: <65, 65–69, 70–79, 80–89, and ≥90 years.
Results : CVC access was associated with the highest mortality. Compared with AVF, CVC was associated with more than a threefold increased mortality risk (adjusted hazard ratio [aHR] 3.54; 95% confidence interval [CI], 3.43–3.65). Though attenuated, risk remained significantly elevated in octogenarians and nonagenarians (aHR 3.30 [95% CI, 3.14–3.47] and 3.18 [95% CI, 2.65–3.82], respectively). Compared with AVG, the risk remained elevated across age groups; however, the survival benefit of AVG over CVC was less pronounced than that of AVF.
Conclusions : CVC use as permanent access was associated with increased mortality, even among the oldest-old adults. AV access should remain the preferred option regardless of age, and CVC access should be reserved for patients with severely limited life expectancy.
Table1.PNG
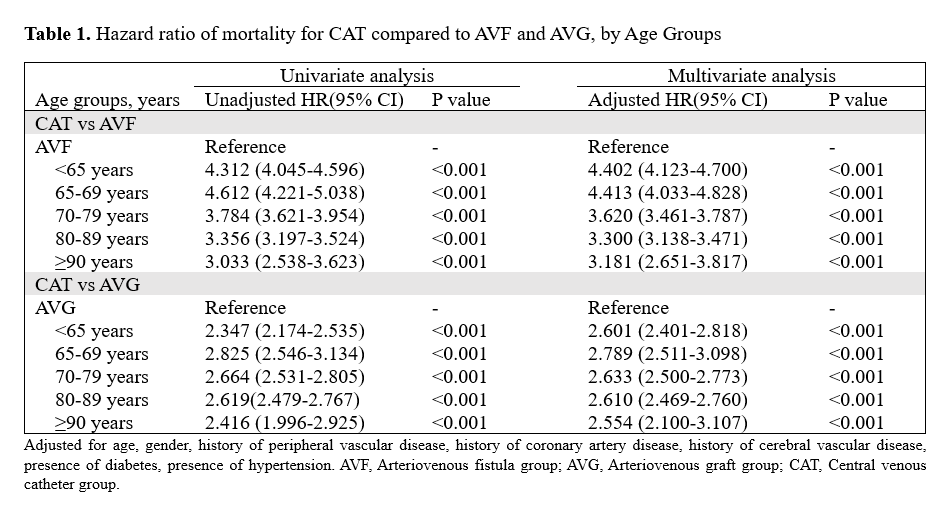
Table1.PNG