Abstract Type : Poster exhibition
Abstract Submission No.: A-0167
Abstract Topic : Non-dialysis CKD
Differential Impact of Chronic Kidney Disease on the Risk of Ischemic Versus Hemorrhagic Stroke
Da Woon Kim1, Jieun Oh2, Whanhee Lee3, Ho Kim2, Dougho Park4, Hyo Jin Kim5
1Department of Internal Medicine-Nephrology, Pusan National University Hospital, Korea, Republic of
2Department of Public Health Science, Graduate School of Public Health, Seoul National University, Korea, Republic of
3Department of Biomedical Convergence Engineering, College of Information and Biomedical Engineering, Pusan National University, Korea, Republic of
4Department of Medical Science and Engineering, Graduate School of Convergence Science and Technology, Pohang University of Science and Technology, Korea, Republic of
5Department of Internal Medicine-Nephrology, Korea University Guro Hospital, Korea, Republic of
Methods : We conducted a retrospective cohort study using the Korean National Health Insurance Service database. A total of 9,909,045 adults aged ≥20 years without prior stroke or renal replacement therapy were followed from 2014 to 2023. CKD was defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m² or relevant diagnostic codes and was further categorized as mild-to-moderate (eGFR 30–59 mL/min/1.73 m²) and advanced (eGFR <30 mL/min/1.73 m²). The primary outcome was incident acute stroke requiring hospitalization with neuroimaging, classified as ischemic or hemorrhagic. Multivariable Cox proportional hazards models adjusted for demographic factors, health behaviors, and comorbidities were used to estimate adjusted hazard ratios (aHRs). Competing risk analyses were performed treating death as a competing event.
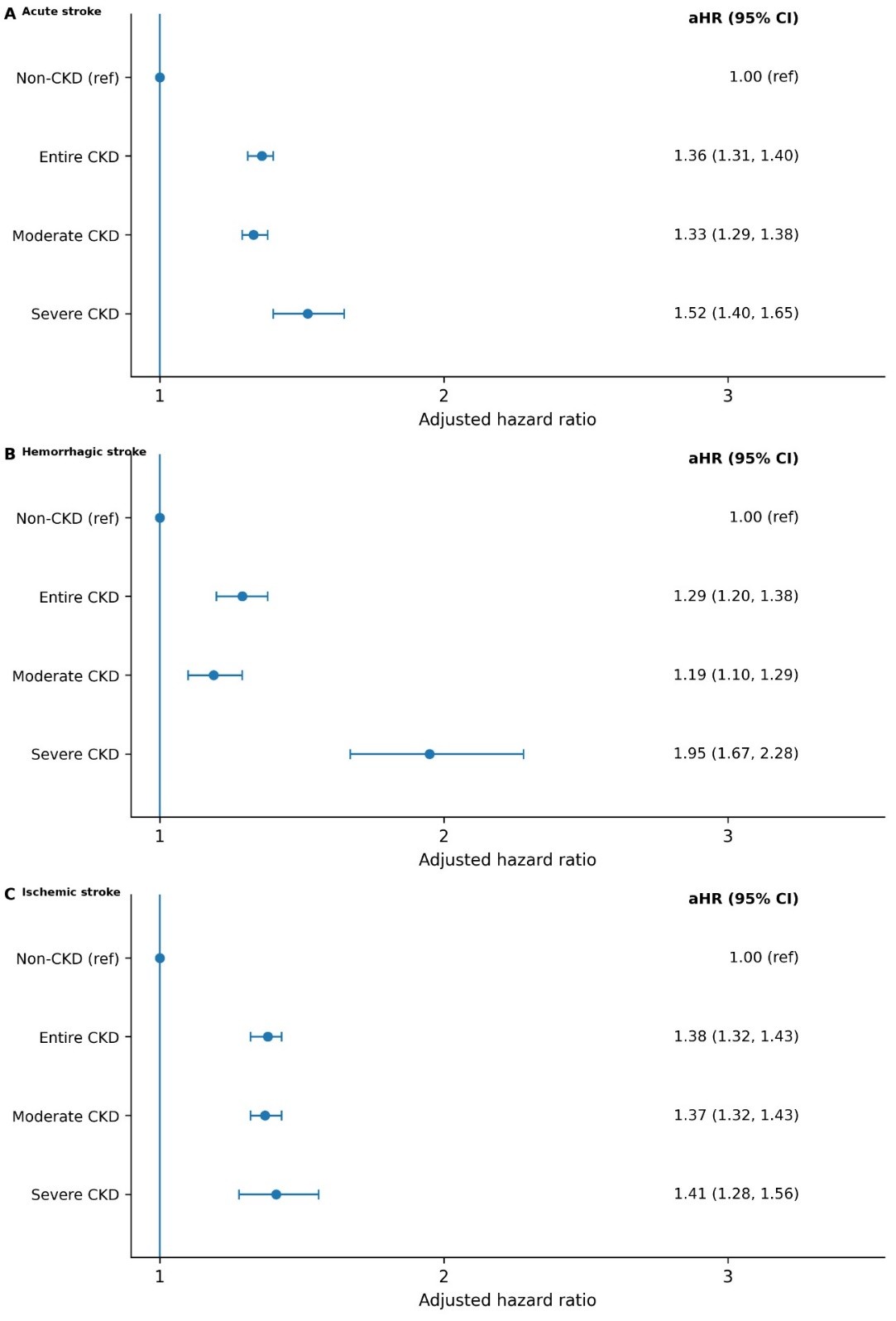
Results : CKD was associated with increased risks of both stroke subtypes, but with distinct risk gradient. For ischemic stroke, the risk increased in participants with moderate CKD (aHR, 1.37 [95% CI, 1.32-1.43]) and showed a small amount of increase in the risk of ischemic stroke in those with advanced CKD (aHR, 1.41 [95% CI, 1.28-1.56]). In contrast, the risk of hemorrhagic stroke exhibited a disproportionate surge in advanced CKD (aHR, 1.95 [95% CI, 1.67-2.28]) compared with moderate CKD (aHR, 1.19 [95% CI, 1.10-1.29]). Competing risk analyses confirmed that advanced CKD remained a strong independent predictor of hemorrhagic stroke (subdistribution HR, 1.83 [95% CI, 1.58-2.13]), indicating that the findings were not driven by survival bias.
Conclusions : CKD was associated with higher risks of ischemic and hemorrhagic stroke, with distinct severity-dependent risk gradient and heterogeneous risk-factor patterns. These findings support subtype-specific and severity-stratified approaches to stroke prevention in patients with CKD.
Figure 1.jpg