Abstract Type : Oral presentation
Abstract Submission No.: A-0112
Abstract Topic : Dialysis
Continuous Intradialytic ECG Surveillance Reveals AF/AFL Burden and Mortality Risk in Hemodialysis
Donghwan Yun, Seung Seok Han
Department of Internal Medicine-Nephrology, Seoul National University Hospital, Korea, Republic of
Objectives : Patients receiving hemodialysis (HD) are predisposed to atrial arrhythmias, but the intradialytic burden of atrial fibrillation/flutter (AF/AFL) and its hemodynamic correlates are not well quantified.
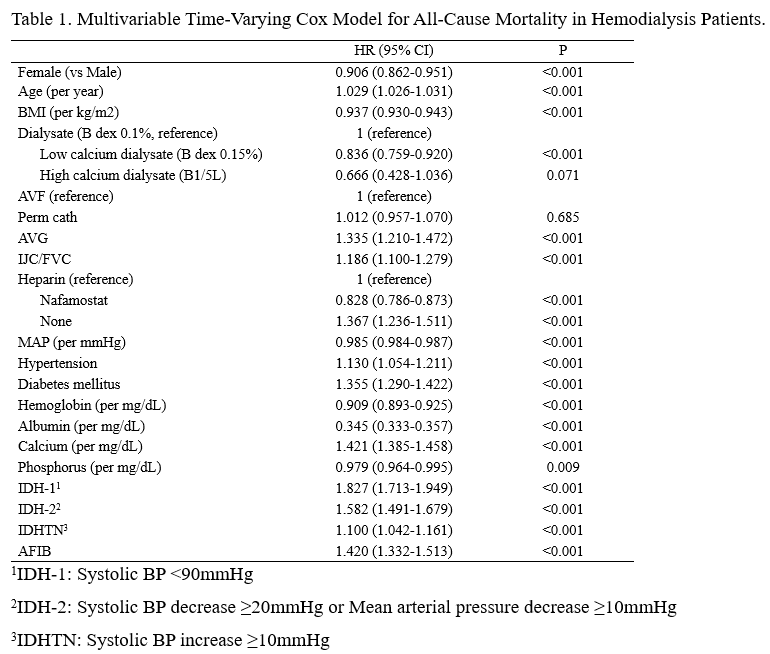
Methods : We retrospectively analyzed intradialytic Lead II ECG recordings from HD sessions between August 2020 and December 2024. Sessions lasting 1–6 h were eligible; recordings <1 h, poor-quality signals (flat ≥50%), and pacemaker sessions were excluded. AF burden was defined as the proportion of each session labeled as AF. All-cause mortality was evaluated using patient-level time-varying Cox models, and intradialytic hypotension/hypertension (IDH-1: SBP<90 mmHg; IDH-2: SBP decrease ≥20 mmHg or MAP decrease ≥10 mmHg; IDHTN: SBP increase ≥10 mmHg) using generalized estimating equation logistic models clustered by patient.
Results : Of 16,808 candidate sessions, 12,925 sessions from 2,760 patients were analyzed; AF was identified in 1,835 sessions (415 patients). Compared with non-AF sessions, AF sessions occurred in older patients with higher comorbidity burden and lower intradialytic MAP. AF was independently associated with increased all-cause mortality (adjusted HR 1.420, 95% CI 1.332–1.513). Mortality risk rose with AF burden (vs 0%): HR 1.280 for burden >0%–<100% and HR 1.538 for burden 100%; low-burden AF (<12.2%) was not clearly associated with mortality, whereas higher burdens were. AF burden <100% was associated with greater odds of intradialytic hypotension, particularly IDH-2, while persistent AF (100% burden) showed no independent association with IDH and AF burden was not associated with IDHTN.
Conclusions : Continuous intradialytic ECG monitoring reveals substantial AF/AFL burden in HD and demonstrates a dose-dependent association with mortality. The linkage between nonpersistent AF and intradialytic hypotension supports hemodynamic instability as a potential trigger and highlights AF burden as a clinically actionable marker for risk stratification and targeted monitoring during HD.
Methods : We retrospectively analyzed intradialytic Lead II ECG recordings from HD sessions between August 2020 and December 2024. Sessions lasting 1–6 h were eligible; recordings <1 h, poor-quality signals (flat ≥50%), and pacemaker sessions were excluded. AF burden was defined as the proportion of each session labeled as AF. All-cause mortality was evaluated using patient-level time-varying Cox models, and intradialytic hypotension/hypertension (IDH-1: SBP<90 mmHg; IDH-2: SBP decrease ≥20 mmHg or MAP decrease ≥10 mmHg; IDHTN: SBP increase ≥10 mmHg) using generalized estimating equation logistic models clustered by patient.
Results : Of 16,808 candidate sessions, 12,925 sessions from 2,760 patients were analyzed; AF was identified in 1,835 sessions (415 patients). Compared with non-AF sessions, AF sessions occurred in older patients with higher comorbidity burden and lower intradialytic MAP. AF was independently associated with increased all-cause mortality (adjusted HR 1.420, 95% CI 1.332–1.513). Mortality risk rose with AF burden (vs 0%): HR 1.280 for burden >0%–<100% and HR 1.538 for burden 100%; low-burden AF (<12.2%) was not clearly associated with mortality, whereas higher burdens were. AF burden <100% was associated with greater odds of intradialytic hypotension, particularly IDH-2, while persistent AF (100% burden) showed no independent association with IDH and AF burden was not associated with IDHTN.
Conclusions : Continuous intradialytic ECG monitoring reveals substantial AF/AFL burden in HD and demonstrates a dose-dependent association with mortality. The linkage between nonpersistent AF and intradialytic hypotension supports hemodynamic instability as a potential trigger and highlights AF burden as a clinically actionable marker for risk stratification and targeted monitoring during HD.
figure1.png
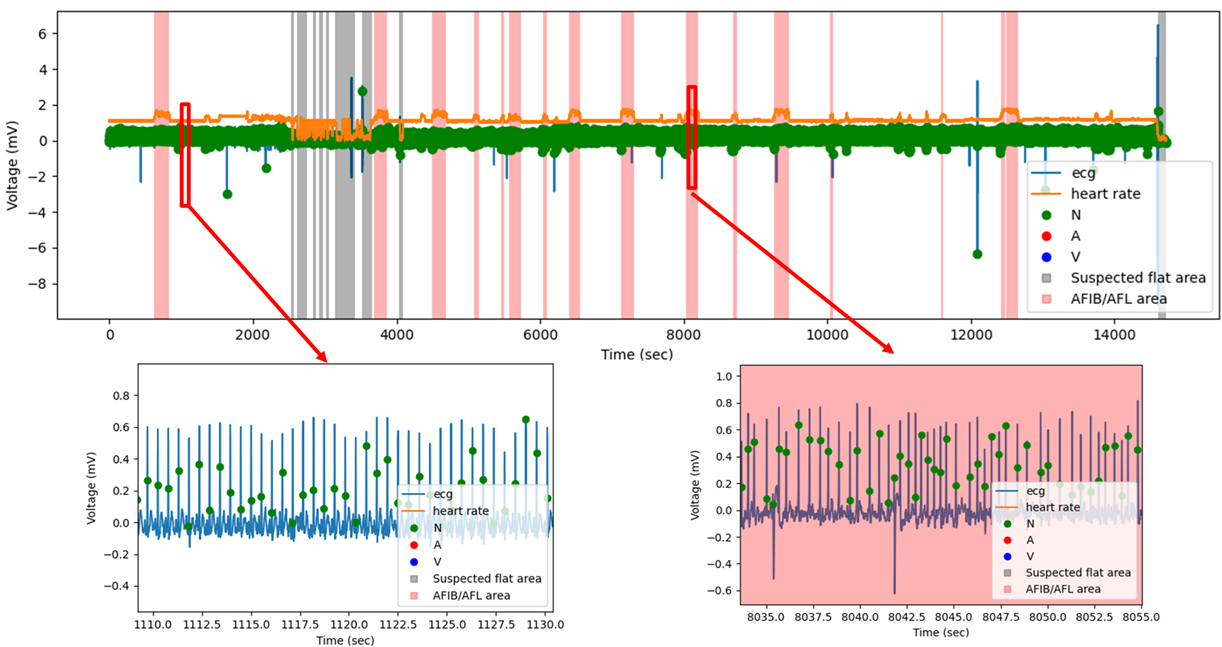
figure1.png