Abstract Type : Oral presentation
Abstract Submission No.: A-0068
Abstract Topic : Transplantation
A Time-to-Equivalent Risk (TiTER) for Decision-Making in Deceased Donor Kidney Transplant Candidates
Omi NA1, Jaeseok Yang2, Jin Hyeog Lee2
1Department of Internal Medicine-Nephrology, Severance Hospital, Korea, Republic of
2Department of Internal Medicine-Nephrology, Catholic Kwandong University International St. Mary's Hospital, Korea, Republic of
Objectives : A US study proposed concept of Time-to-Equivalent Risk (TiTER) as a decision-making tool for accepting organs from expanded criteria donors. While this study demonstrated a higher initial cumulative incidence of deceased donor kidney transplantation (DDKT) than death, the applicability and pattern of TiTER may differ in regions with extreme organ scarcity, such as Korea.
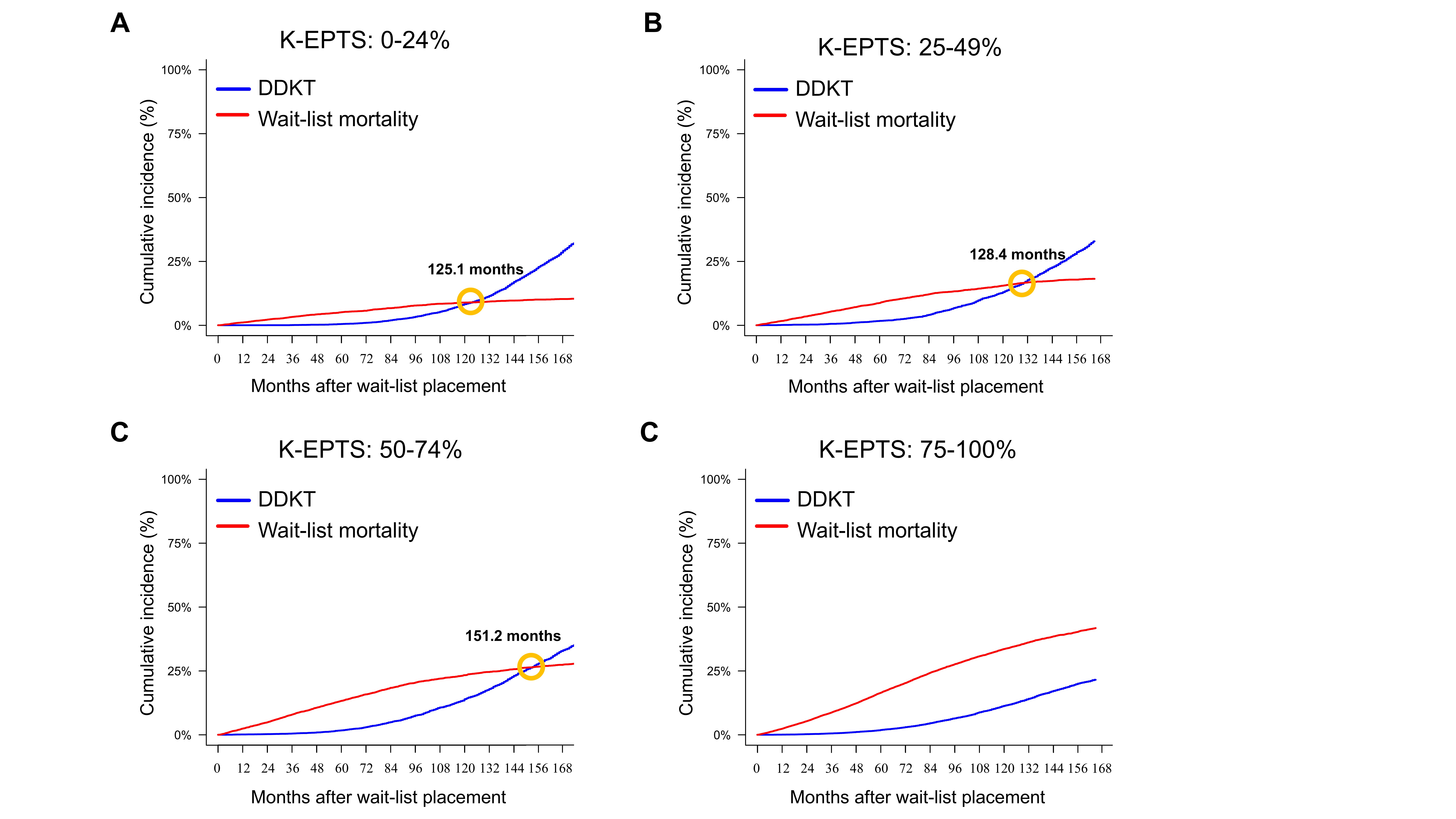
Methods : Using comprehensive, nationwide cohort data from the Korean Network for Organ Sharing registry and National Health Insurance (2008-2022, n=51,427), we analyzed the cumulative incidence and competing risks of DDKT versus wait-list mortality, estimating the Korean TiTER (K-TiTER). Analyses were stratified by recipient age, Korean Estimated Post-Transplant Survival (K-EPTS), blood type, and donor quality.
Results : Among 53,650 waitlisted patients, 10,603 (20%) received DDKT. The cumulative incidence of DDKT was initially lower than that of death, in the opposite pattern to the US study. Therefore, K-TiTER was defined as the earliest time when DDKT probability exceeds wait-list mortality. K-TiTER in the overall cohort was 240.3 months. Among candidates aged ≥65 years, those with high K-EPTS scores (75–100), or blood type O, K-TiTER was frequently not reached, as the wait-list mortality consistently exceeded transplant probability. Notably, sensitivity analyses showed that expanding donor acceptance criteria shortened the time to risk-benefit crossover. This finding reframes suboptimal donor organs as a strategic accelerator for mitigating wait-list mortality, especially in candidates with poor prognosis.
Conclusions : K-TiTER provides practical guidance for identifying vulnerable candidates and implementing preferential allocation of high-risk organs to high-risk recipients or enrollment in an innovative clinical trial.
Methods : Using comprehensive, nationwide cohort data from the Korean Network for Organ Sharing registry and National Health Insurance (2008-2022, n=51,427), we analyzed the cumulative incidence and competing risks of DDKT versus wait-list mortality, estimating the Korean TiTER (K-TiTER). Analyses were stratified by recipient age, Korean Estimated Post-Transplant Survival (K-EPTS), blood type, and donor quality.
Results : Among 53,650 waitlisted patients, 10,603 (20%) received DDKT. The cumulative incidence of DDKT was initially lower than that of death, in the opposite pattern to the US study. Therefore, K-TiTER was defined as the earliest time when DDKT probability exceeds wait-list mortality. K-TiTER in the overall cohort was 240.3 months. Among candidates aged ≥65 years, those with high K-EPTS scores (75–100), or blood type O, K-TiTER was frequently not reached, as the wait-list mortality consistently exceeded transplant probability. Notably, sensitivity analyses showed that expanding donor acceptance criteria shortened the time to risk-benefit crossover. This finding reframes suboptimal donor organs as a strategic accelerator for mitigating wait-list mortality, especially in candidates with poor prognosis.
Conclusions : K-TiTER provides practical guidance for identifying vulnerable candidates and implementing preferential allocation of high-risk organs to high-risk recipients or enrollment in an innovative clinical trial.
Figure1_KSN.jpg
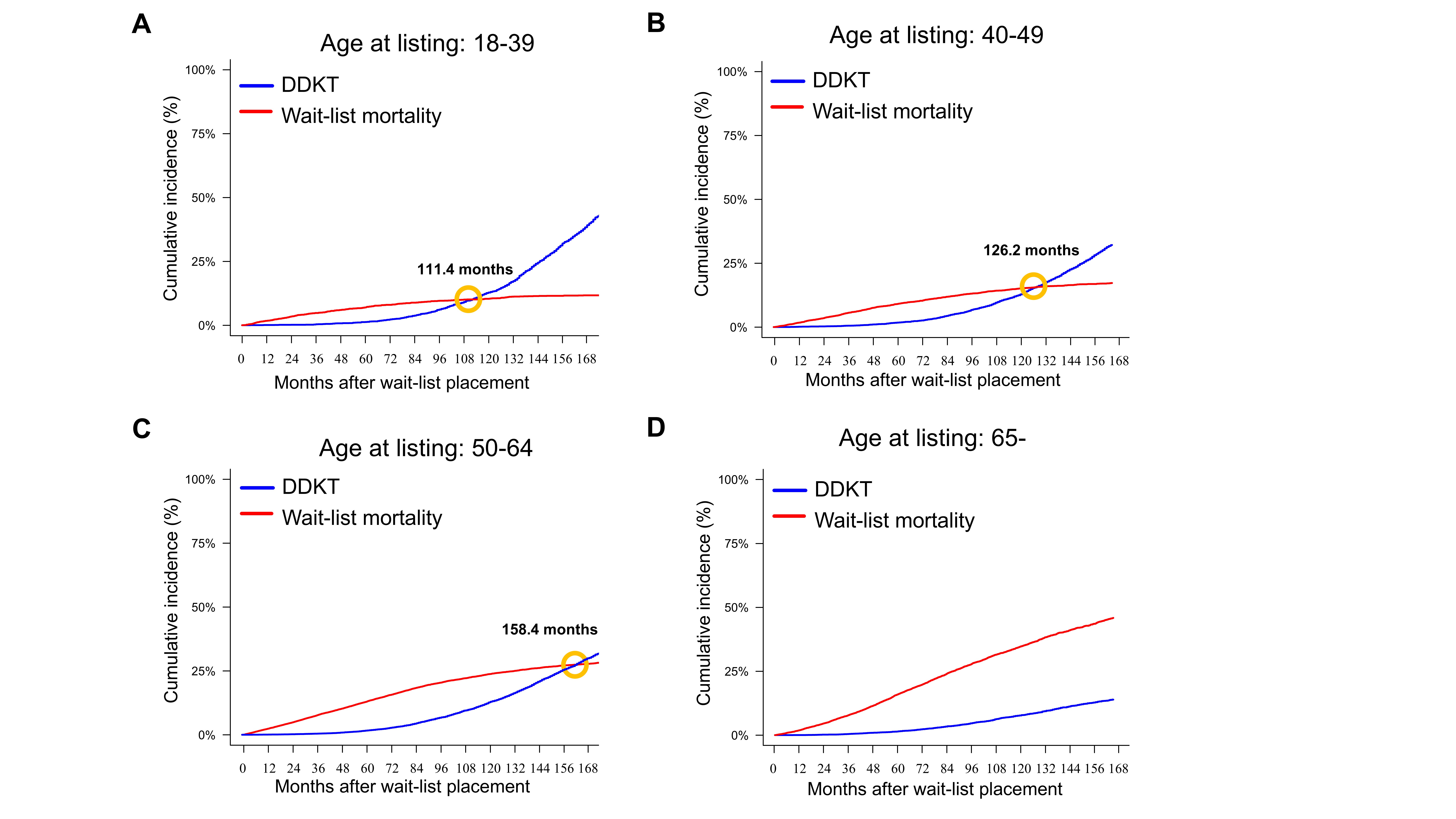
Figure1_KSN.jpg